Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Microemboli: revisione
M. Del Sette Dipartimento di Neuroscienze Università di Genova

2
IPOTESI CLINICA GLI EVENTI CEREBROVASCOLARI SONO IN MAGGIOR PARTE DI ORIGINE EMBOLICA IL DOPPLER TRANSCRANICO PUO’ RILEVARE MICROEMBOLI ( M.E.S.) 3. LA MICROEMBOLIA E’ CORRELATA ALLA MACROEMBOLIA

3
SOMMARIO COME SI FA LA DIAGNOSI DI M.E.S.?
IN QUALI CONDIZIONI CLINICHE SI POSSONO RILEVARE? SONO INFLUENZATI DA TERAPIE? DI COSA SONO COMPOSTI?

4
(Consensus Committee, Stroke’95 and ‘98)
DIAGNOSI DI M.E.S. Durata < 300 msec. Ampiezza > 3 dB Unidirezionalità Suono tipico Monitoraggio prolungato (Consensus Committee, Stroke’95 and ‘98)
")
5
CONDIZIONI CLINICHE CON PRESENZA DI M.E.S.
1. STENOSI CAROTIDEA 2. PATOLOGIE CARDIACHE EMBOLIGENE 3. ICTUS ISCHEMICO ACUTO 4. INTERVENTI DI ENDOARTERIECTOMIA CAROTIDEA - ANGIOPLASTICA E STENT 5. CHIRURGIA CARDIACA

6
MES SONO MARKER SURROGATO DI EVENTI?

7
FATTORI DI RISCHIO PER: ICTUS M.E.S.
entità della stenosi carotidea placca ulcerata pregresso TIA sintomi recenti presenza di M.E.S.? entità della stenosi carotidea placca ulcerata pregresso TIA sintomi recenti

8
M.E.S. E STENOSI CAROTIDEA
(Siebler et al., ’94)
")
9
Valore predittivo dei M.E.S.
111 PAZIENTI STENOSI >60% MES: 41 (36.9%) STENOSI: <70: 22% 70-90: 48% >90: 21% RECIDIVA PIU’ FREQUENTE IN STENOSI CON M.E.S: O.R. 8.10 (Molloy and Markus, 1999)
 STENOSI: <70: 22% 70-90: 48% >90: 21% RECIDIVA PIU’ FREQUENTE IN STENOSI CON M.E.S: O.R (Molloy and Markus, 1999)")
11
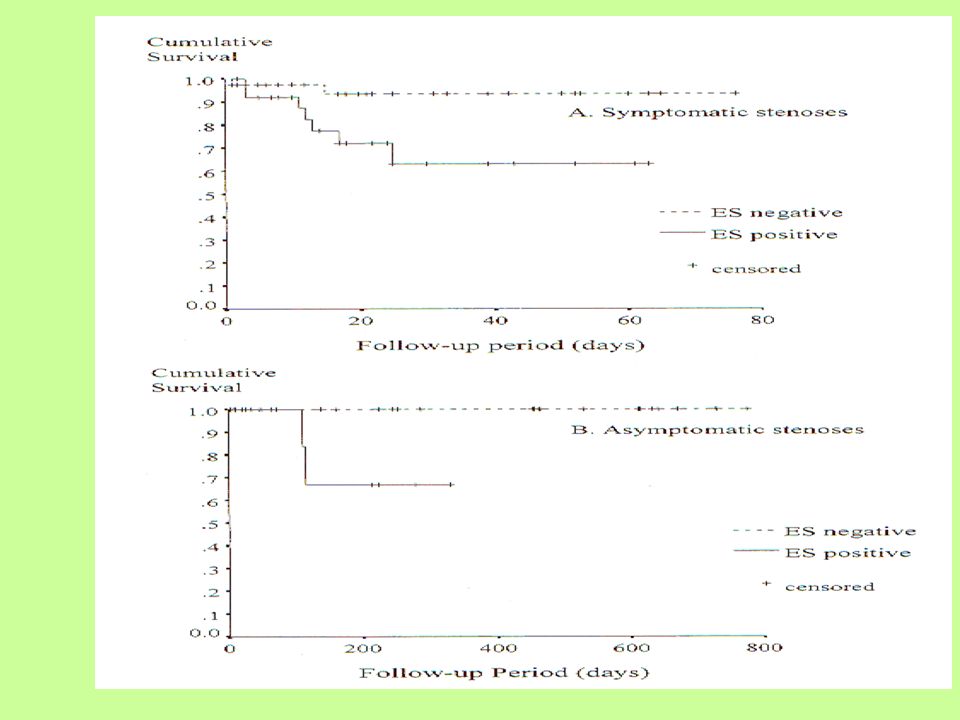
M.E.S.: marker di eventi clinici nella stenosi carotidea>60%
MES criteria Patients Risk of Stroke/TIA* MES positive Symptomatic1 X 8 With >1 MES per hour Symptomatic and asymptomatic2 X 9 With >2 MES per hour Symptomatic3 X 31 1.Siebler M et al. Stroke 1995; 26: 21842186. 2. Valton L et al. Stroke 1998; 29: 21252128. 3. Molloy J et al. Stroke 1999; 30: 14401443.

12
Stenosi asintomatiche senza MES sono a basso rischio
Monitoraggio per 1 ora in 2 occasioni MES in 32 (10%) A 1 anno: rischio di ictus 15.6% vs. 1% (p<.0001) (Spence et al., Stroke 2005;36:2373-8)
 A 1 anno: rischio di ictus 15.6% vs. 1% (p<.0001) (Spence et al., Stroke 2005;36:2373-8)")
13
Significato prognostico dei M.E.S. nell’ictus acuto
Nessuna relazione con prognosi funzionale Possibile significato predittivo sulla probabilità di recidiva precoce (Valton et al., ‘97; Babikian et al., ‘97) Correlati con deterioramento cognitivo (Russell, ’92)
 Correlati con deterioramento cognitivo (Russell, ’92)")
14
MES POSSONO ESSERE USATI PER STUDIARE L’EFFETTO DI FARMACI?

15
Cardioembolie Nessuna correlazione tra MES e terapie (anticoagulanti o antiaggreganti) Georgiadis et al., Anticoagulation monitoring with transcranial Doppler.Lancet ;344(8933):1373-4 Sturzenegger et al., Monitoring Combined Antithrombotic Treatments in Patients With Prosthetic Heart Valves Using Transcranial Doppler and Coagulation Markers Stroke. 1995;26:63-69 Sliwka et al., Occurrence of Transcranial Doppler High-Intensity Transient Signals in Patients With Potential Cardiac Sources of Embolism Stroke. 1995;26: ‘98, Del Sette et al., Warfarin, aspirin and microembolic signals in the acute phase of stroke in a patient with mechanical heart valves. Cerebrovasc Dis (3):182-3
: Sturzenegger et al., Monitoring Combined Antithrombotic Treatments in Patients With Prosthetic Heart Valves Using Transcranial Doppler and Coagulation Markers Stroke. 1995;26: Sliwka et al., Occurrence of Transcranial Doppler High-Intensity Transient Signals in Patients With Potential Cardiac Sources of Embolism Stroke. 1995;26: ‘98, Del Sette et al., Warfarin, aspirin and microembolic signals in the acute phase of stroke in a patient with mechanical heart valves. Cerebrovasc Dis (3):")
16
Ictus acuto No correlazione tra MES e ASA, eparina o warfarin
Georgiadis et al., Anticoagulation monitoring with transcranial Doppler.Lancet ;344(8933):1373-4 Tong et al., Transcranial Doppler–Detected Microemboli in Patients With Acute Stroke. Stroke. 1995;26: Del Sette et al. Microembolic Signals With Serial Transcranial Doppler Monitoring in Acute Focal Ischemic Deficit A Local Phenomenon? Stroke.1997;28: Poppert et al.Embolic signals in unselected stroke patients Stroke 2006;37: )
: Tong et al., Transcranial Doppler–Detected Microemboli in Patients With Acute Stroke. Stroke. 1995;26: Del Sette et al. Microembolic Signals With Serial Transcranial Doppler Monitoring in Acute Focal Ischemic Deficit A Local Phenomenon Stroke.1997;28: Poppert et al.Embolic signals in unselected stroke patients Stroke 2006;37: )")
17
Sliwka et al. Prevalence and Time Course of Microembolic Signals in Patients With Acute Stroke (Stroke. 1997;28: )
.")
18
ICTUS ACUTO: ANEDDOTICA
1 case of MCA stenosis: disappearance of after Warfarin + ticlopidine (Segura et al., ’98) 1 case of PCA infarction: MES disappearance after Warfarin + ASA (Behrens et al., ’99) 1 case of basilar stenosis: reduction of MES after warfarin (Kassnasrallah et al., ’99) 2 reports: decline of MES after heparine (Dinia et al. Cerebrovasc Dis. 2006; Marinoni et al., Eur Neurol ‘06)
 1 case of PCA infarction: MES disappearance after Warfarin + ASA (Behrens et al., ’99) 1 case of basilar stenosis: reduction of MES after warfarin (Kassnasrallah et al., ’99) 2 reports: decline of MES after heparine (Dinia et al. Cerebrovasc Dis. 2006; Marinoni et al., Eur Neurol ‘06)")
19
(Goertler et al.,Stroke. 1999;30:66-69.)
STENOSI CAROTIDEA 9 pt. with recently symptomatic ICA stenosis: ASA i.v. (500 mg): significant reduction of ipsilateral MES in 7 after 30 minutes no ischemic event was observed within a 90-day follow-up after the initiation of ASA prevention compared with 2.3 events in the month before. (Goertler et al.,Stroke. 1999;30:66-69.)
: significant reduction of ipsilateral MES in 7 after 30 minutes. no ischemic event was observed within a 90-day follow-up after the initiation of ASA prevention compared with 2.3 events in the month before. (Goertler et al.,Stroke. 1999;30:66-69.)")
20
(Goertler et al., Cerebrovasc Dis ’01)
STENOSI CAROTIDEA 74 pt., 1 hour monitoring 26 without ASA: 73% MES 48 with ASA: 40% Predictors of MES: Absence of ASA (OR 7.1; 95% CI ) Recurrent events (OR 3.8; 95% CI ) (Goertler et al., Cerebrovasc Dis ’01) (p=0.023)
 Recurrent events (OR 3.8; 95% CI ) (Goertler et al., Cerebrovasc Dis ’01) (p=0.023)")
21
STENOSI ACI O ACM 8 pt.with recent (7 days) TIA and ASA therapy
Addition of clopidogrel and MES monitoring from 3rd to 7th days Significant decrease of MES (cessation in 4) (Esagunde et al., Cerebrovasc Dis, 2006)
 (Esagunde et al., Cerebrovasc Dis, 2006)")
22
CARESS Randomized, controlled, double blind (n=107)
Clopidogrel 75 mg o.d. Clopidogrel 300 mg Clopidogrel n = 50 R ASA 75 mg o.d. to all patients from D1 to D7±1 Placebo n = 50 Placebo Placebo o.d. MES detection MES detection MES detection (Markus et al., Circulation, 2005)
")
23
CARESS: Results (Markus et al., Circulation, 2005) RRR 25.2% p = 0.078
Primary Endpoint Results: Number of MES+ Patients at D7** 100% 100% 100 80 76.0% 72.5% 56.8% % of Patients 60 45.5% 40 Placebo* Clopidogrel* 20 Baseline Day 1 Day 7 (Markus et al., Circulation, 2005)
")
24
ASA + CLOPIDOGREL CHE FARE?
MATCH N= 7599 TIA (21%) or stroke (79%) + 1 RF Distance from symptoms: 3 months F.U.: 18 months many lacunar stroke CARESS N= 107 TIA (63%) or stroke (37%) Distance from symptoms: 3 months F.U.: 7 days all > 50% carotid stenosis
 or stroke (79%) + 1 RF. Distance from symptoms: 3 months. F.U.: 18 months. many lacunar stroke. CARESS. N= 107. TIA (63%) or stroke (37%) Distance from symptoms: 3 months. F.U.: 7 days. all > 50% carotid stenosis.")
25
NATURA DEI M.E.S. Gassosa Particolata (piastrine, trombo)
")
26
NATURA DEI M.E.S. Inalazione ossigeno Rete neurale
Analisi multifrequenza: 2 MHz riflette gas 2.5 MHz riflette particelle solide Analisi “time frequency” (wavelet transform)
")
27
CONCLUSIONI - I M.E.S. INDICANO LA PRESENZA NEL VASO DI MATERIALE A IMPEDENZA DIFFERENTE DAL SANGUE COMPOSTI DA GAS O PARTICELLE MARKER DI EVENTI CLINICI, SPECIE IN STENOSI CAROTIDEA

28
CONCLUSIONI - II NECESSITANO DI TECNICHE DI MONITORAGGIO PROLUNGATO (60’) ICTUS ACUTO: predittori di recidiva e deterioramento cognitivo MONITORAGGIO ENDOARTERIECTOMIA E STENTING

29
GRAZIE

Presentazioni simili



















 RELATORE DR. ADOLFO.>")