Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
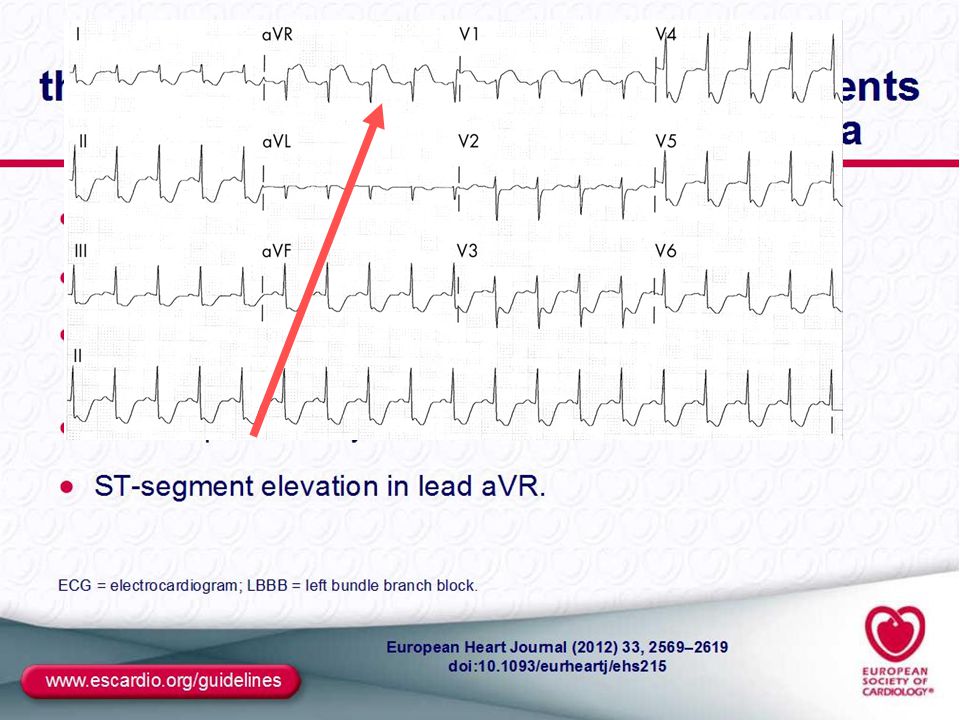
Management dell’Infarto Miocardico Acuto a presentazione “sopralivellamento del tratto ST”
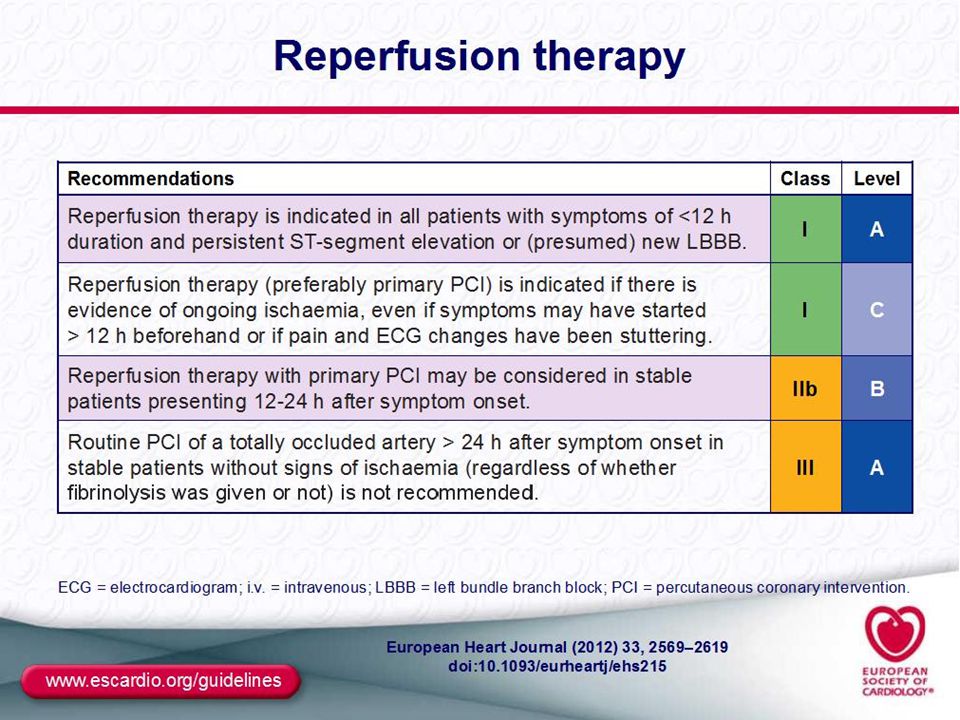
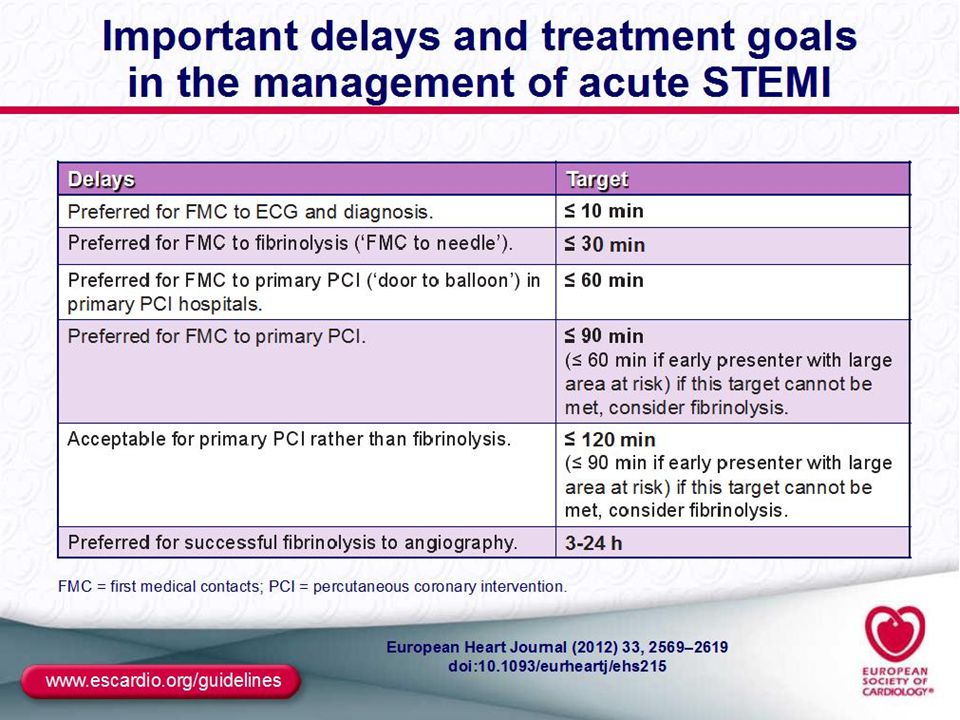
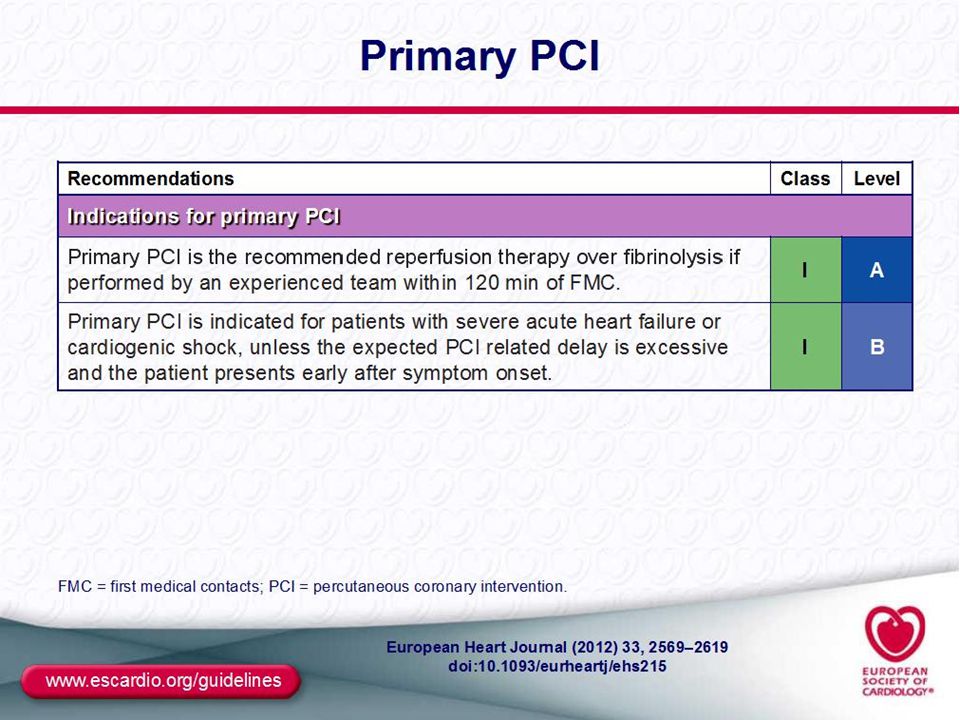
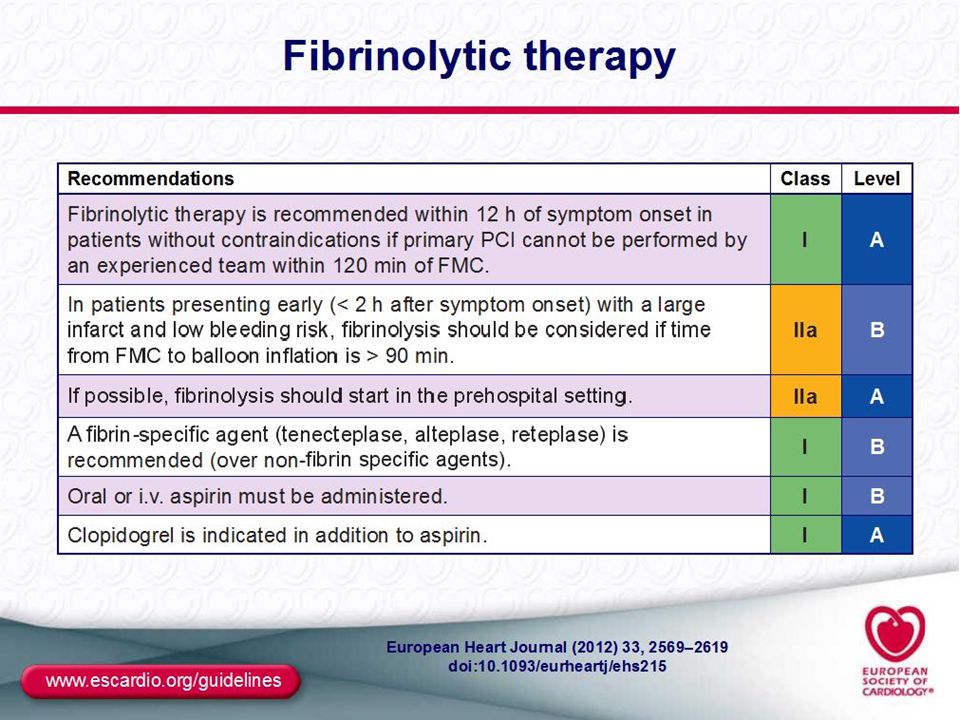
STEMI Linee Guida ESC 2012

12
Time to Reperfusion and Outcome
20 40 60 80 100 1 3 6 12 12-24 % Extent of salvage (% of area at risk) Mortality reduction (%) A-B – no benefit Potential outcomes D B-C – benefit ? C A-C – benefit D-C – harm B A Time to treatment is critical Opening the IRA PPCI>lysis Gersh JAMA 2005 La partia si gioca entro le 3 ore modello sperimentale di ischemia che evolve in necrosi ttransmurale ma la realtà è diversa in ogni singolo caso. Basta pensare alla chiusura INTERMITTENTE , EVOLUZIONE DI PLACCA SU ISCHEMIA CRONICA (PRECONDIZIONAMENTO) , COLLATERALIZZAZIONE CHE ALLRGA LA FINESTRA DI ISCHEMIA PIUTTOSTO CHE DI NECROSI
 Mortality reduction (%) A-B – no benefit. Potential outcomes. D. B-C – benefit C. A-C – benefit. D-C – harm. B. A. Time to treatment is critical. Opening the IRA PPCI>lysis. Gersh JAMA La partia si gioca entro le 3 ore modello sperimentale di ischemia che evolve in necrosi ttransmurale ma la realtà è diversa in ogni singolo caso. Basta pensare alla chiusura INTERMITTENTE , EVOLUZIONE DI PLACCA SU ISCHEMIA CRONICA (PRECONDIZIONAMENTO) , COLLATERALIZZAZIONE CHE ALLRGA LA FINESTRA DI ISCHEMIA PIUTTOSTO CHE DI NECROSI.")
13
Tcheng J Am Coll Cardiol 48:1336, 2006
UN PASSO INDIETRO ED UNO SGUARDO AL PASSATO. SENZA ENTRARE NEL DETTAGLIO Tcheng J Am Coll Cardiol 48:1336, 2006

15
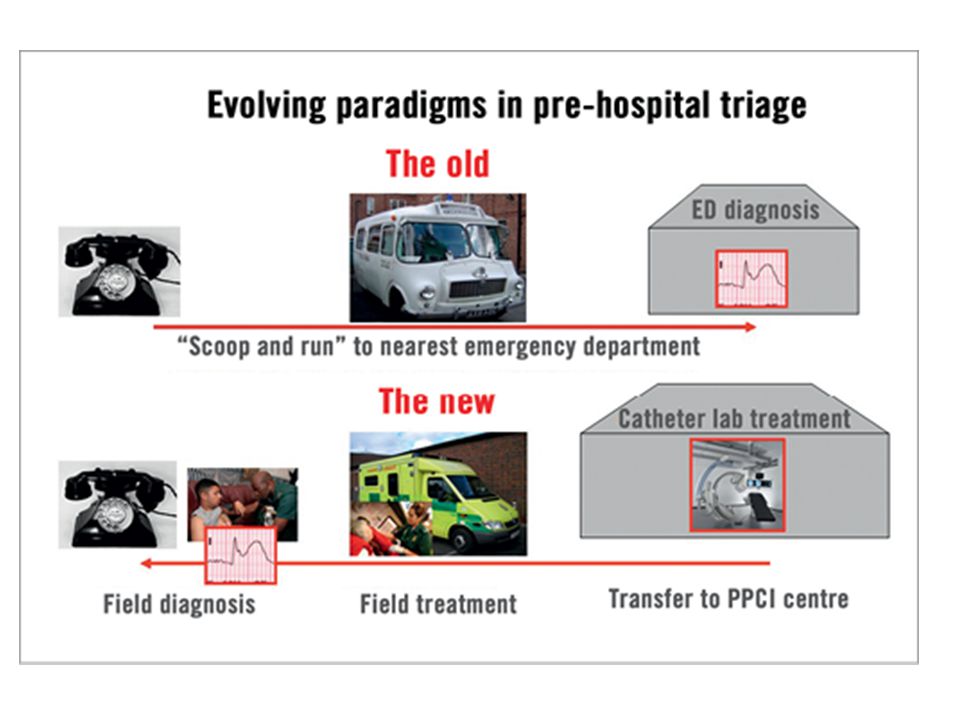
Hospital based concept
Team approach Patient public important link of the chain : calling help integral with cath lab activation EMS trained , outreach arm of H attack centre protocols

18
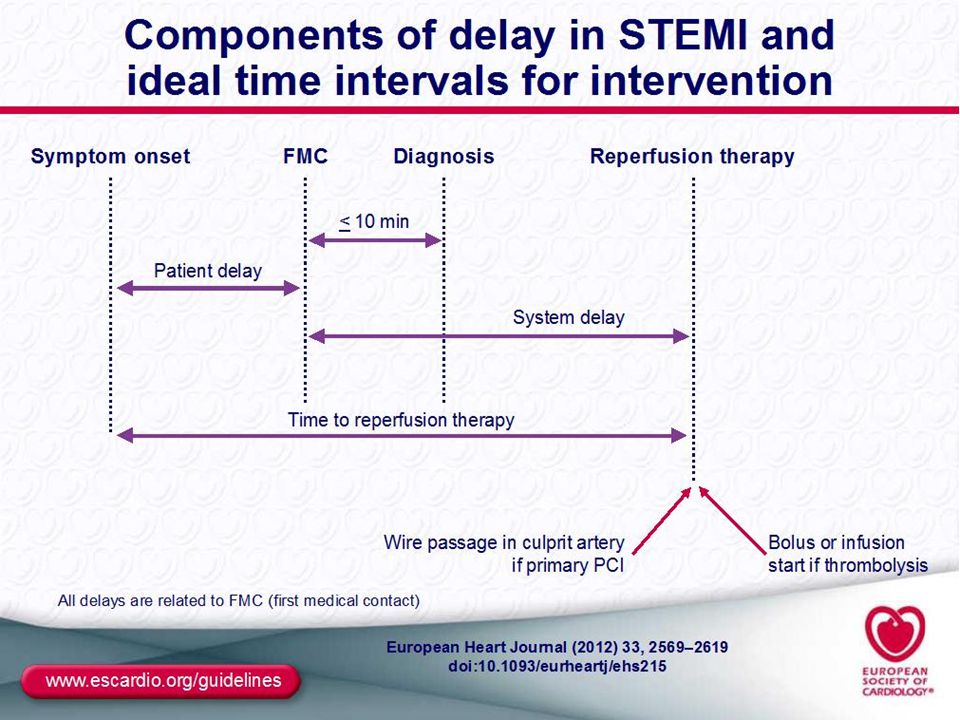
Modificabile da provvedimenti organizzativipiù del patient delay
Indicatore di qualità Entro 90 dal FMC (vero D2B) entro 60 in ospedale capace di PPCI
 entro 60 in ospedale capace di PPCI.")
19
System delay ALGORITMO system delay dalla diagnosi STEMI (FMC):non sempre vero
:non sempre vero")
20
Patient Delay Algoritmo contenente patient delay, dall’esordio dei sintomi alla riperfusione tempo totale ischemico

21
Ecg teletrasmesso certificazione di qualità perché valutato dal cardiologo.
Nella ns realtà da quel momento la cardiologia è allertata: il cardiologo UTIC /la cardiologia nella validazione diagnostica attiva emodinamista (condivide il caso) , posto letto
 , posto letto.")
22
Direttamente in sala emodinamica
Protocollo condiviso Monitoraggio continuo Commenti linee guida alala luce della loro applicazione locale . Se ci guardiamo indietro 7-8 aa fa iniziammo la trasmissione tt avanguardia di rete (NB a FI non esiste) Il confronto migliora la qualità del sistema emergenza e se non è possibile trasmettere non perdere tempo Direttamente in sala emodinamica Bypass DEA
 Il confronto migliora la qualità del sistema emergenza e se non è possibile trasmettere non perdere tempo. Direttamente in sala emodinamica. Bypass DEA.")
23
Percoso STEMI pistoia Accesso diretto sala per 1PTCA Cardiologo UTIC
FMC Diagnosi Ecg teletrasmesso Trasporto monitoraggio Accesso diretto sala per 1PTCA Percorso+ attivazione sala Emodinamista reperibile & staff : infermiere/TRS Ritardo di sistema

24
173 64 26 83 STEMI ENTRO 12 ORE ANNO 2012 173 N.TOTALE PAZIENTI
RESCUE POST-TL 173 PCI PRIMARIA 64 37% 26 15% 83 48% DIRETTA AL CL TRASFERITA DA SPOKE AMMESSA AD HUB

25
D2B TOTALE PAZIENTI N. 173 N. PAZIENTI 173 – MEDIANA D2B: 90 MINUTI
PER D2B SI INTENDE DAL PRIMO CONTATTO MEDICO AL PRIMO PAASAGGIO DI MATERIALE ATTO A RIPERFONDERE IL VASO IN SALA. QUINDI è UN TEMPO COMPLESSIVO, NON DI TRASFERIMENTO AL LABORATORIO, NELLE LINEE GUIDA è SCRITTO di eseguire PTCA ENTRO 90 MIN (FINO A 120) ma non chiarisce mai bene se è incluso il tempo d sala o l’arrivo alla sala. Qui in tempo di sala (mediana circa 20 min) è incluso. PAZIENTI
 ma non chiarisce mai bene se è incluso il tempo d sala o l’arrivo alla sala. Qui in tempo di sala (mediana circa 20 min) è incluso. PAZIENTI.")
26
D2B AMMISSIONE DIRETTA 118 N. PAZIENTI 64 – MEDIANA D2B: 84 MINUTI

27
D2B AMMISSIONE PS PO PISTOIA
N. PAZIENTI 47 – MEDIANA D2B: 90 MINUTI

28
D2B AMMISSIONE PS PO PESCIA
N. PAZIENTI 45 – MEDIANA D2B: 100 MINUTI MINUTI 28

29
PCI di trasferimento tra PO
N. PAZIENTI 26 – MEDIANA D2B: 125 MINUTI MINUTI TUTTI I PAZIENTI TRASFERITI DA UN PO ALL’ALTRO PER ESEGUIRE LA PROCEDURA, SIA ACCETTATI IN DEA CHE PROVENIENTI DAI REPARTI, SIA VERSO PESCIA CHE VERSO PT, INCLUSI ANCHE I PAZIENTI DA SANMARCELLO (N.5) PAZIENTI
 PAZIENTI.")
30
Oltre il 50% della mortalità totale di IMA è preospedaliera
Oltre il 50% della mortalità totale di IMA è preospedaliera .Nel patient delay è raccolta una gran parte dei casi di MI allorche all’esordio dell’ima la disomogeneita elettrica è massima e conseguentemente la vulnerabilita ad FV . Attivazione team anestesiologico che assiste il pz in sala emodinamica – Se IOT ventilazione .ipotermia terapeutica

36
Motality benefit of primary PCI declines with “PCI-related time delay”
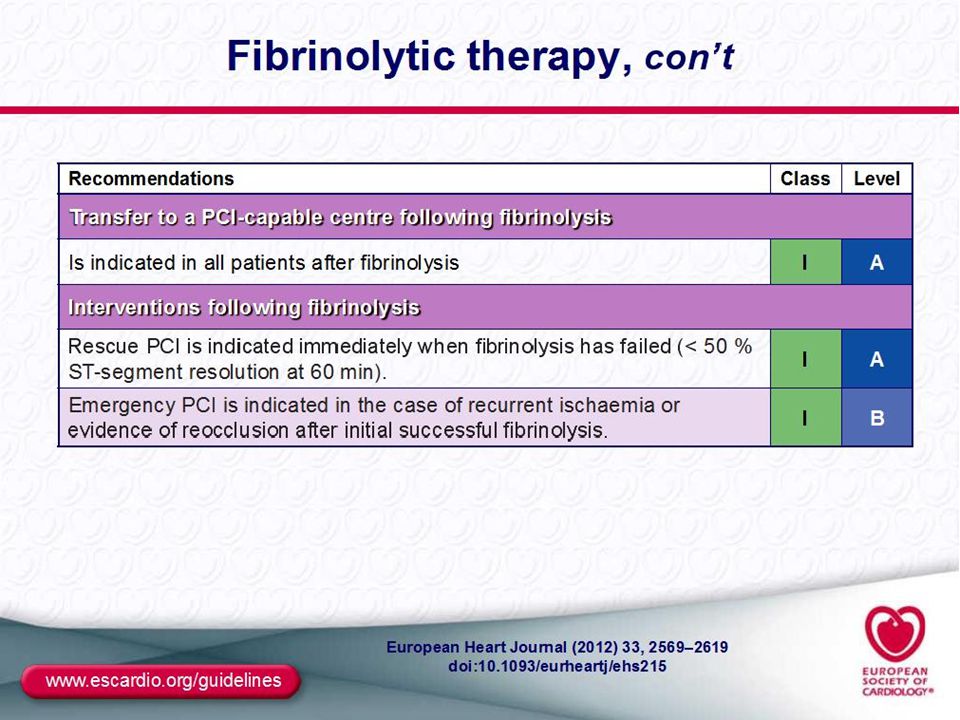
10 − 13 RCTs N = 5494 P = 0.04 5 − Favors PCI Mortality equipose: 60 min Absolute Risk Difference in Death (%) 0 − A decision must be made when a STEMI patient presents to a center without interventional cardiology facilities. Fibrinolytic therapy can generally be provided sooner than primary PCI. As the time delay for performing PCI increases, the mortality benefit associated with expeditiously performed primary PCI over fibrinolysis decreases. Compared with a fibrin-specific lytic agent, a PCI strategy may not reduce mortality when a delay greater than 60 minutes is anticipated versus immediate administration of a lytic, as shown in this figure. Favors fibrinolysis with a fibrin-specific agent -5 − ┬ ┬ ┬ ┬ ┬ ┬ PCI-Related Time Delay (minutes) Nallamothu and Bates. Am J Cardiol 2003;92:824.
 0 − A decision must be made when a STEMI patient presents to a center without interventional cardiology facilities. Fibrinolytic therapy can generally be provided sooner than primary PCI. As the time delay for performing PCI increases, the mortality benefit associated with expeditiously performed primary PCI over fibrinolysis decreases. Compared with a fibrin-specific lytic agent, a PCI strategy may not reduce mortality when a delay greater than 60 minutes is anticipated versus immediate administration of a lytic, as shown in this figure. Favors fibrinolysis with a fibrin-specific agent. -5 − ┬ ┬ ┬ ┬ ┬ ┬ PCI-Related Time Delay (minutes) Nallamothu and Bates. Am J Cardiol 2003;92:824.")
38
BACKGROUND Large contemporary international registries continue to demonstrate persisting delays to primary PCI in STEMI patients first presenting to EMS or non-cath capable hospitals Subsequent transfer for primary PCI commonly results in reperfusion times exceeding current guideline recommendations These delays are associated with commensurate increases in morbidity and mortality

39
STUDY AIM A strategy of early fibrinolysis followed by coronary angiography within 6-24 hours or rescue PCI if needed was compared with standard primary PCI in STEMI patients with at least 2 mm ST-elevation in 2 contiguous leads presenting within 3 hours of symptom onset and unable to undergo primary PCI within 1 hour.

40
STUDY PROTOCOL After 20% of the planned recruitment, the TNK dose was reduced by 50% among patients ≥75 years of age. STEMI <3 hrs from onset symptoms, PPCI <60 min not possible, 2 mm ST-elevation in 2 leads RANDOMIZATION 1:1 by IVRS, OPEN LABEL Strategy A: pharmaco-invasive Strategy B: primary PCI Ambulance/ER <75y:full dose ≥75y: ½ dose TNK no lytic Aspirin Clopidogrel: LD 300 mg + 75 mg QD Enoxaparin: 30 mg IV + 1 mg/kg SC Q12h Aspirin Clopidogrel: 75 mg QD Enoxaparin: 0.75 mg/kg SC Q12h Antiplatelet and antithrombin treatment according to local standards ECG at 90 min: ST resolution ≥ 50% PCI Hospital YES NO angio >6 to 24 hrs PCI/CABG if indicated immediate angio + rescue PCI if indicated Standard primary PCI Primary endpoint: composite of all cause death or shock or CHF or reinfarction up to day 30

41
MEDIAN TIMES TO TREATMENT (min)
1st Medical contact Randomize IVRS Sx onset Rx TNK 62 29 9 100 min 78 min difference 1st Medical contact Sx onset Randomize IVRS Rx PPCI 61 31 86 1 Hour 2 Hours n=1892 178 min

42
MEDIAN TIMES TO TREATMENT (min)
1st Medical contact Randomize IVRS Sx onset Rx TNK 36% Rescue PCI at 2.2h 62 29 9 100 min 64% non-urgent cath at 17h 1st Medical contact Sx onset Randomize IVRS Rx PPCI 61 31 86 1 Hour 2 Hours 178 min n=1892

43
Dth/Shock/CHF/ReMI (%)
PRIMARY ENDPOINT TNK vs PPCI Relative Risk 0.86, 95%CI ( ) PPCI 14.3% TNK 12.4% p=0.24 Dth/Shock/CHF/ReMI (%) The 95% CI of the observed incidence in the pharmaco-invasive arm would exclude a 9% relative excess compared with PPCI
 PPCI 14.3% TNK 12.4% p=0.24. Dth/Shock/CHF/ReMI (%) The 95% CI of the observed incidence in the pharmaco-invasive arm would exclude a 9% relative excess compared with PPCI.")
44
STROKE RATES Pharmaco-invasive PPCI P-value TOTAL POPULATION (N=1892)
Total stroke fatal stroke Haemorrhagic stroke fatal haemorrhagic stroke 15/939 (1.60%) 7/939 (0.75%) 9/939 (0.96%) 6/939 (0.64%) 5/946 (0.53%) 4/946 (0.42%) 2/946 (0.21%) 0.03 0.39 0.04 0.18 POST AMENDMENT POPULATION (N=1503) 9/747 (1.20%) 3/747 (0.40%) 4/747 (0.54%) 2/747 (0.27%) 5/756 (0.66%) 4/756 (0.53%) 2/756 (0.26%) 0.30 >0.999 0.45
 7/939 (0.75%) 9/939 (0.96%) 6/939 (0.64%) 5/946 (0.53%) 4/946 (0.42%) 2/946 (0.21%) POST AMENDMENT POPULATION (N=1503) 9/747 (1.20%) 3/747 (0.40%) 4/747 (0.54%) 2/747 (0.27%) 5/756 (0.66%) 4/756 (0.53%) 2/756 (0.26%) >")
48
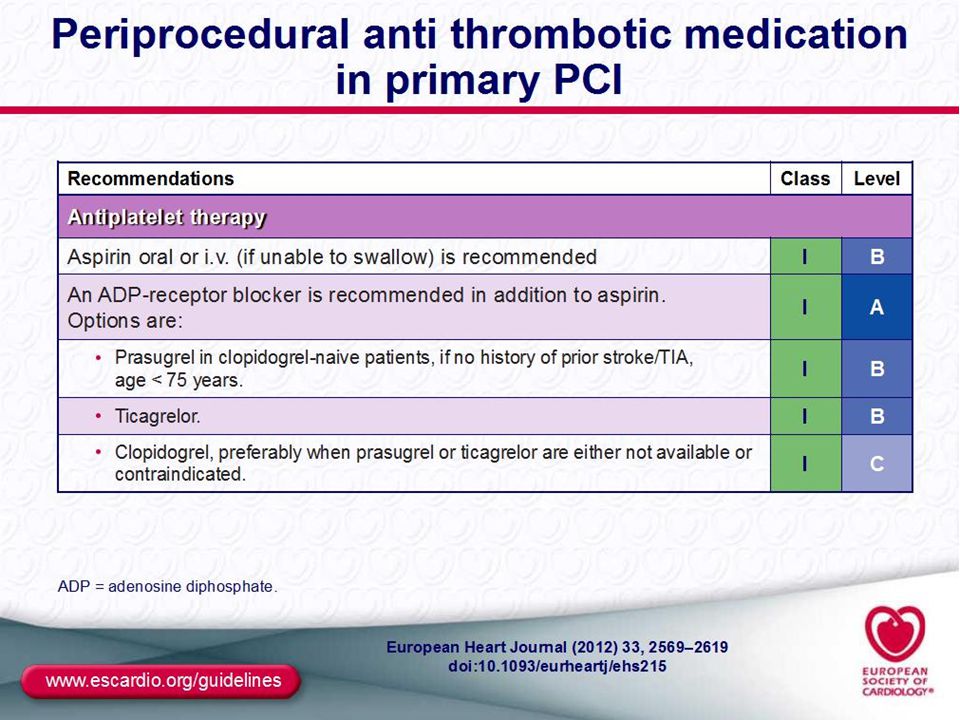
Bleeding Risk Subgroups Therapeutic Considerations
Reduced MD Guided by PK Age > 75 or Wt < 60 kg Avoid Prasugrel Prior CVA/TIA 16% 4% Significant Net Clinical Benefit with Prasugrel 80% MD 10 mg 48 48

49
Timing of Benefit (Landmark Analysis)
8 6.9 Clopidogrel Clopidogrel 6 5.6 5.6 Primary Endpoint (%) 4.7 4 Prasugrel Prasugrel HR 0.82 P=0.01 HR 0.80 P=0.003 2 1 1 2 3 30 60 90 180 270 360 450 Days Loading Dose Maintenance Dose 49
 Prasugrel. Prasugrel. HR 0.82 P=0.01. HR 0.80 P= Days. Loading Dose. Maintenance Dose. 49.")
51
PLATO - STEMI substudy - Outcomes
Time-related Kaplan–Meier estimates of the time to first occurrence of the primary end point (incidence of MI, stroke, or vascular death; HR, 0.87; 95% CI, 0.75 to 1.01; P=0.07) Steg P.G., et al. Circulation 2010;122: 51
 Steg P.G., et al. Circulation 2010;122:")
Presentazioni simili







 Metanalysis Davide.>")






 al PS circa il 5% delle prestazioni>")
 sottoposto a CABG.>")








