Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
Sorveglianza Epidemiologica Regionale delle Malattie Cardiovascolari
Dr. Enrico Balli ASL 3 Area Pistoiese Emodinamica Aziendale - U.O. Cardiologia Pistoia 16 febbraio 2008

2
Indicatori di malattia
1° Campagna Educazionale Regionale ANMCO Toscana Indicatori di malattia Per descrivere le malattie cardiovascolari si utilizzano i seguenti indicatori: prevalenza proporzione di pazienti portatori della malattia cardiovascolare mortalità n° decessi in un determinato intervallo di tempo

3
letalità proporzione di decessi
1° Campagna Educazionale Regionale ANMCO Toscana letalità proporzione di decessi nei malati incidenza n° nuovi casi per anno tasso di attacco n° di eventi nella popolazione, incluse le ricadute

4
Fonti dei dati nazionali
1° Campagna Educazionale Regionale ANMCO Toscana Fonti dei dati nazionali prevalenza Osservatorio Epidemiologico Cardiovascolare (ISS – ANMCO) mortalità Banca dati mortalità ISS letalità e tasso di attacco Registro nazionale degli eventi coronarici e cerebrovascolari incidenza Progetto MONICA-OMS
 mortalità Banca dati mortalità ISS. letalità e tasso di attacco. Registro nazionale degli eventi. coronarici e cerebrovascolari. incidenza Progetto MONICA-OMS.")
5
Fonti dei dati regionali
1° Campagna Educazionale Regionale ANMCO Toscana Fonti dei dati regionali Registro di Mortalità Regionale Schede di Dimissione Ospedaliera Registro Regionale dell’Infarto Miocardico Acuto

6
Sorveglianza epidemiologica regionale delle malattie cardiovascolari
1. Conoscenze su distribuzione ed andamento fattori di rischio 2. Conoscenze su frequenza ed andamento diverse forme morbose

7
Effect of risk factors/ treatments on CHD mortality
CHD deaths prevented or postponed by risk factor changes and treatments in England and Wales, 1981 to 2000 10,000 e.g. diabetes, obesity Risk factors: worse 13% –10,000 Risk factors: better 71% e.g. smoking, cholesterol, BP –20,000 Deaths prevented or postponed in 2000 –30,000 Treatments 42% –40,000 68,230 fewer deaths in 2000 e.g. secondary prevention, heart failure treatments –50,000 2,888 more deaths due to diabetes 2,662 more deaths due to physical inactivity 2,097 more deaths due to obesity –60,000 –70,000 1981 Year 2000 Unal B, Circulation 2004; 109:1101–1107

8
Lowering of the Cholesterol Level Control of Blood Pressure
Cessation of Smoking Lowering of the Cholesterol Level Control of Blood Pressure Avoidance of Obesity Maintenance of Normal Glucose Tolerance Maintenance of a Physically Active Lifestyle Mild to Moderate Consumption of Alcohol JE Manson et al, N Engl J Med 1992: 326 (21);
;")
9
Sedentary lifestyle / Physical inactivity
Relative risk of death from coronary heart disease twice (1.9, CI ) in sedentary as compared with active people 45% lower risk of myocardial infarction for those who maintan an active as compared with a sedentary lifestyle JE Manson et al, N Engl J Med 1992: 326 (21);
 in sedentary as compared with active people. 45% lower risk of myocardial infarction for those who maintan an active as compared with a sedentary lifestyle. JE Manson et al, N Engl J Med 1992: 326 (21);")
10
Avoidance of Obesity Obese (BMI >29) have a 3.3 (CI ) relative risk of coronary heart disease Overweights (BMI 25-29) have a 80% increase in risk Weight gain >10 kg between early and mid adulthood doubles the risk Distribution of fat: abdomen, upper body Maintenance of an ideal body weight as compared with being obese (>20% above desiderable body weight)reduces the risk of MI by 35-55% JE Manson et al, N Engl J Med 1992: 326 (21);
 have a 80% increase in risk. Weight gain >10 kg between early and mid adulthood doubles the risk. Distribution of fat: abdomen, upper body. Maintenance of an ideal body weight as compared with being obese (>20% above desiderable body weight)reduces the risk of MI by 35-55% JE Manson et al, N Engl J Med 1992: 326 (21);")
11
The Metabolic Syndrome
Abdominal obesity - Waist circumference Men > 102 cm Women > 88 cm Elevated triglycerides > 150 mg/dl Low HDL-cholesterol Men < 40 mg/dl Women <50 mg/dl Raised blood pressure >130/85 mmHg Fasting glucose > 110 mgdl Gotto AM. Eur Heart J 2002; 4 (F): F 7 – 11.
: F 7 – 11.")
12
Alcohol consumption Mild to moderate reduces the risk of MI by 25-45%
“Moderate” oz (350 cc) beer, one glass of wine, one drink of hard liquor daily Benefit indipendent of the type of beverage Heavy users have an increased risk of myocardial infarction stroke and mortality from coronary heart disease The difference between drinking small to moderate quantities of alcohol and drinking large amounts may mean the difference between preventing and causing disease JE Manson et al, N Engl J Med 1992: 326 (21);
 beer, one glass of wine, one drink of hard liquor daily. Benefit indipendent of the type of beverage. Heavy users have an increased risk of myocardial infarction stroke and mortality from coronary heart disease. The difference between drinking small to moderate quantities of alcohol and drinking large amounts may mean the difference between preventing and causing disease. JE Manson et al, N Engl J Med 1992: 326 (21);")
13
Type D (distressed type) personality trait
4-fold increase of death in patients with established CAD Social inhibition (inhibition of self-expression) Negative affectivity (negative emotions) Chronic suppression of emotions Correlates Emotional stress Worry, gloomy view of life, unhappy irritated Keeps others at distance Inhibits expression of true feelings Social Depression Chronic tension Low subjective well being Low levels of perceived social support Psychometric Denollet J et al. Lancet 1996; 347:
 Negative affectivity (negative emotions) Chronic suppression. of emotions. Correlates. Emotional stress. Worry, gloomy. view of life, unhappy. irritated. Keeps others at distance. Inhibits expression of. true feelings. Social. Depression. Chronic tension. Low subjective. well being. Low levels of. perceived social. support. Psychometric. Denollet J et al. Lancet 1996; 347:")
14
“.. (at present) the evidence of an association between religion, spirituality and health is weak and inconsistent ..” “..No-one can object to respectful support for patients who draw upon religious faith in times of illness. However, until these ethical issues are resolved, suggestions that religious activity will promote health, that illness is the result of insufficient faith, are unwarranted.” Sloan RP. Religion, spirituality and medicine. Lancet 1999; 353:

15
Smoking… More than doubles the incidence of coronary heart disease
Increases mortality from coronary heart disease by 70% Current smokers: dose /response relation between the number of cigarettes smoked and heart disease Ex-smokers: within two to three years after they quit the risk of myocardial infarction declines to levels similar to those of never-smokers 50-70% estimated reduction in the risk of myocardial infarction with cessation of smoking JE Manson et al, N Engl J Med 1992: 326 (21);
;")
16
Lowering of the Cholesterol Level
Relative Risk Estimated reduction in the risk of myocardial infarction 2-3% for each 1% reduction in serum cholesterol level JE Manson et al, N Engl J Med 1992: 326 (21);
;")
17
Control of Blood Pressure
Relative Risk Estimated reduction in the risk of myocardial infarction 2-3% for each decline of 1 mmHg in diastolic blood pressure JE Manson et al, N Engl J Med 1992: 326 (21);
;")
18
Diabetes mellitus A statement for Healthcare professionals from AHA and ACC Scott M. Grundy, MD, et al. Circulation 1999 “.....Thus diabetes must take its place alongside the other major risk factors as importance causes of CVD.....it may be appropriate to say - diabetes is a cardiovascular disease - ...”

19
Intermittent claudication
Framingham Heart Study 30-Year Follow-Up: CVD Events in Patients With Diabetes (Ages 35-64) 10 Men Women 8 Risk ratio 6 4 * 2 Total CVD CHD Cardiac failure Intermittent claudication Stroke Age-adjusted annual rate/1,000 P<0.001 for all values except *P<0.05 Wilson PWF, Kannel WB. In: Hyperglycemia, Diabetes and Vascular Disease. Ruderman N et al, eds. Oxford; 1992.
 10. Men. Women. 8. Risk. ratio * 2. Total CVD. CHD. Cardiac failure. Intermittent claudication. Stroke. Age-adjusted annual rate/1,000. P<0.001 for all values except *P<0.05. Wilson PWF, Kannel WB. In: Hyperglycemia, Diabetes and Vascular Disease. Ruderman N et al, eds. Oxford;")
20
Colditz GA, Rimm EB, Giovannucci E,
A prospective study of parental history of myocardial infarction and coronary artery disease in men. Colditz GA, Rimm EB, Giovannucci E, Stampfer MJ, Rosner B, Willett WC. Am J Cardiol May 1;67(11):933-8. Compared with men without any history of parental MI, those whose mothers or fathers had had an MI at less than 70 years of age had a substantially elevated risk of MI (relative risk = 2.2, 95% confidence interval, 1.2 to 3.8 for maternal history; relative risk = 1.7, 95% confidence interval 1.2 to 2.3 for paternal history). Risk of MI increased with decreasing age at parental MI.
: Compared with men without any history of parental MI, those whose mothers or fathers had had an MI at less than 70 years of age had a substantially elevated risk of MI (relative risk = 2.2, 95% confidence interval, 1.2 to 3.8 for maternal history; relative risk = 1.7, 95% confidence interval 1.2 to 2.3 for paternal history). Risk of MI increased with decreasing age at parental MI.")
21
PROCARDIS: A current approach to the study of the genetics of myocardial infarct.
Barlera S, Chiodini B, Franzosi MG, Tognoni G. Ital Heart J Suppl Sep;2(9): PROCARDIS Consortium Genome-wide mapping of susceptibility to coronary artery disease identifies a novel replicated locus on chromosome 17. PLoS Genet May;2(5):e72. Epub 2006 May 19
: PROCARDIS Consortium. Genome-wide mapping of susceptibility to coronary artery disease identifies a novel replicated locus on chromosome 17. PLoS Genet May;2(5):e72. Epub 2006 May 19.")
22
Jackson R, et al. Lancet 2005; 365: 434-41

23
ISTAT – Indagini multiscopo
Conoscenze su distribuzione ed andamento fattori di rischio Abitudine al fumo Toscana: % fumatori MASCHI FEMMINE Toscana Italia Toscana Italia Fumatori correnti % % % % Ex fumatori % % % % Mai fumato % % % % ISTAT – Indagini multiscopo

24
ISTAT – Indagine multiscopo - 2005
Conoscenze su distribuzione ed andamento fattori di rischio Attività fisica maschi femmine ISTAT – Indagine multiscopo

25
ISTAT – Indagine multiscopo – 2005
Conoscenze su distribuzione ed andamento fattori di rischio Indice massa corporea maschi femmine ISTAT – Indagine multiscopo – 2005 > 18 anni

26
Sorveglianza epidemiologica regionale delle malattie cardiovascolari
Conoscenze su frequenza ed andamento diverse forme morbose Mortalità Ricoveri ospedalieri Uso farmaci Registro toscano Infarto miocardico acuto Registro toscano Eventi cerebrovascolari acuti

27
Mortalità

28
Infarto Miocardico 26% eventi: decessi prima del ricovero
Azienda USL Eventi Ospedalizzati Morti senza Ricovero Massa Carrara 522 152 Lucca 501 177 Pistoia 513 279 Prato 401 131 Pisa 624 290 Livorno 1.041 326 Siena 548 232 Arezzo 654 204 Grosseto 644 194 Firenze 1.641 560 Empoli 386 126 Viareggio 485 135 Area Vasta CENTRO 2.941 1.096 NORD-OVEST 3.173 1.080 SUD-EST 1.846 630 Toscana 7.960 2.806 Eventi ospedalizzati e morti senza ricovero : Toscana, Aree Vaste e Aziende USL Numero casi . Anno 2004 26% eventi: decessi prima del ricovero 1 decesso extra osp. ogni 2.8 casi ospedalizzati Pistoia: peso decessi extraospedalieri elevato

29
Ictus Cerebrale Azienda USL Eventi Ospedalizzati Morti senza ricovero
Eventi ospedalizzati e morti senza ricovero : Toscana Aree Vaste ed Aziende USL – Numero casi Anno 2004 Azienda USL Eventi Ospedalizzati Morti senza ricovero Massa e Carrara 485 79 Lucca 827 84 Pistoia 604 91 Prato 544 70 Pisa 849 107 Livorno 872 119 Siena 754 96 Arezzo 945 108 Grosseto 646 78 Firenze 2.283 198 Empoli 597 81 Viareggio 380 57 Area Vasta CENTRO 4.028 440 NORD-OVEST 3.413 446 SUD-EST 2.345 282 Toscana 9.786 1.168 Le morti senza ricovero hanno una rilevanza meno importante di quella osservata a proposito dell’ infarto del miocardio . Rappresentano circa l’ 11% del totale dei casi incidenti ; 1 decesso extraospedaliero ogni 9 casi ospedalizzati

30
ARS – Relazione Sanitaria regionale 2003-2005
Conoscenze su frequenza ed andamento diverse forme morbose Pazienti in trattamento con farmaci antiipertensivi anno 2005 21.6% pistoiesi 21% toscani ARS – Relazione Sanitaria regionale

31
Registri di popolazione
Obiettivo : raccolta sistematica e continuativa di tutti i casi di una specifica malattia che insorgono in una determinata popolazione, definita in base all’area di residenza . Informazioni sulle caratteristiche della malattia in vari sottogruppi della popolazione residente nell’area di rilevazione e sulle variazioni geografiche e temporali di incidenza, prevalenza e sopravvivenza

32
Registri di popolazione
Un registro di popolazione deve assicurare il rispetto di determinati standard di qualità dei dati raccolti, in particolare deve garantire - chiari criteri di diagnosi - la completezza della raccolta dei casi (arruolamento di ogni caso insorto nella specifica popolazione, evitando doppie registrazioni e l’inclusione di pazienti non elegibili ad es. per la residenza ) - la completezza e l’accuratezza delle informazioni fondamentali (es. età e sesso)
 - la completezza e l’accuratezza delle informazioni fondamentali (es. età e sesso)")
33
Tosc-AMI Registro Toscano dell’Infarto Miocardico Acuto
Valutazione frequenza e prognosi degli episodi di IMA verificatisi tra i residenti della regione Trattamento fase acuta della malattia - PTCA e Coronarografia Mortalità : Registro di Mortalità Regionale gestito dal CSPO attraverso schede ISTAT ASL 2 U.O.Cardiologia - Zona Valle del Serchio

34
Incidenza dell’infarto miocardico acuto in Toscana
1° Campagna Educazionale Regionale ANMCO Toscana Incidenza dell’infarto miocardico acuto in Toscana circa eventi ogni anno (59 % dei casi nei maschi) 8.000 (73 %) episodi di IMA ospedalizzato 2.900 (27 %) morti coronariche extraospedaliere Dal 2000 sono in aumento gli eventi ospedalizzati e decrescono le morti coronariche senza ricovero
 (73 %) episodi di IMA ospedalizzato (27 %) morti coronariche extraospedaliere. Dal 2000 sono in aumento gli eventi ospedalizzati e decrescono le morti coronariche senza ricovero.")
35
Tassi per 100.00 abitanti, standardizzati per età. Toscana
Conoscenze su frequenza ed andamento diverse forme morbose Incidenza infarto miocardico acuto Tassi per abitanti, standardizzati per età. Toscana ARS – Registro regionale Infarto Miocardico Acuto

36
Tassi per 100.00 abitanti, standardizzati per età . Toscana
Conoscenze su frequenza ed andamento diverse forme morbose Incidenza infarto miocardico acuto Maschi Tassi per abitanti, standardizzati per età . Toscana ARS – Registro regionale Infarto Miocardico Acuto

37
Tassi per 100.00 abitanti, standardizzati per età . Toscana
Conoscenze su frequenza ed andamento diverse forme morbose Incidenza infarto miocardico acuto Femmine Tassi per abitanti, standardizzati per età . Toscana ARS – Registro regionale Infarto Miocardico Acuto

38
Tassi per 100.00 abitanti, standardizzati per età. Toscana 2003-2005
Conoscenze su frequenza ed andamento diverse forme morbose Incidenza infarto miocardico acuto Maschi Femmine Tassi per abitanti, standardizzati per età. Toscana ARS – Registro regionale Infarto Miocardico Acuto

39
Tassi per 100.00 abitanti, standardizzati per età. Toscana 2003-2005
Conoscenze su frequenza ed andamento diverse forme morbose Incidenza ictus cerebrale Maschi Femmine Tassi per abitanti, standardizzati per età. Toscana ARS – Registro regionale Eventi cerebrovascolari acuti

40
Angioplastica coronarica
Uso PTCA entro il primo giorno dalla data di incidenza dell’ infarto cardiaco (eventi ospedalizzati) in Toscana Andamento temporale – Percentuali standardizzate per età 320 interventi nel 1997 – nel 2005 Maschi 35 % - Femmine 20 % (tale differenza rimane anche dopo l’aggiustamento per l’età )
 in Toscana. Andamento temporale – Percentuali standardizzate per età. 320 interventi nel 1997 – nel Maschi 35 % - Femmine 20 % (tale differenza rimane anche dopo l’aggiustamento per l’età )")
41
Considerazioni conclusive
Sorveglianza epidemiologica regionale delle malattie cardiovascolari Considerazioni conclusive Rilevanza patologia cardiovascolare Trend incidenza “favorevoli” (al netto dell’invecchiamento della popolazione) Siamo in grado di monitorare sufficientemente bene le malattie Insufficiente conoscenza della differente distribuzione dei principali fattori di rischio nelle diverse aree della regione “Difendiamo il cuore” non solo con le terapie ma anche intervenendo sulla modifica delle abitudini di vita!
 Siamo in grado di monitorare sufficientemente bene le malattie. Insufficiente conoscenza della differente distribuzione dei principali fattori di rischio nelle diverse aree della regione. Difendiamo il cuore non solo con le terapie ma anche intervenendo sulla modifica delle abitudini di vita!")
42
Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study INTERHEART. Lancet 2004; 364:

43
Relative risk (RR) – probability of an individual with a risk factor experiencing a coronary event compared with an individual lacking that risk factor Population attributable risk (PAR) percentage – estimate of the % of all cases of coronary artery disease within a population that would be prevented if that risk factor were removed from the population Cowie MR, Eur Heart J 2002; 23:
 percentage – estimate of the % of all cases of coronary artery disease within a population that would be prevented if that risk factor were removed from the population. Cowie MR, Eur Heart J 2002; 23:")
44
Regular physical activity 0.86 12.2 Alcohol consumption (moderate)
RR PAR% Smoking 2.87 35.7 Raised Apo B/ApoA1 3.25 49.2 Hypertension 1.91 17.9 Diabetes 2.37 9.9 Abdominal Obesity 1.62 20.1 Psychosocial factors 2.67 32.5 Regular physical activity 0.86 12.2 Alcohol consumption (moderate) 0.91 6.7 Fruits and vegetables 0.70 13.7 Family history of MI (men, early age) 1.45 9.8 INTERHEART. Lancet 2004; 364:
 Fruits and vegetables Family history of MI (men, early age) INTERHEART. Lancet 2004; 364:")
45
“.. Collectively, these nine risk factors account for 90% of the PAR (population attributable risk) in men – 91.5% including parental history of myocardial infarction at early age – and 94% in women.. ” INTERHEART. Lancet 2004; 364:

46
DART M.L. Burr et al. Lancet 1989; ii:757-61

47
Lyon diet heart study Circulation 1999; 99:733-5. The composite outcome of cardiac death and nonfatal MI was significantly reduced by Mediterranean dietary pattern (14 events vs 44 in the prudent Western-type diet group)
")
48
UKPDS Group, Lancet 1998; 352:

49
UKPDS Group, Lancet 1998; 352:

50
NNT Numero di pazienti da trattare per prevenire un evento 100
Riduzione assoluta del rischio

51
Prevenzione primaria Rid.% eventi coronarici LDL mg/dl Rid.% LDL Rid.%
mortalità NNT WOSCOPS 192 26 22 31 42 AFCAPS TexCAPS 150 25 37 44 Beneficio max per HDL-C < 40 mg/dl Maron DJ, Circulation 2000; 101: 207. 22

52
Heart Protection Study; Lancet. 2002 Jul 6;360(9326):7-22.
:7-22.")
53
Prevenzione primaria HOPE
Ramipril Placebo 14.0 17.8 anni % P<0.001 22% IMA, stroke, mortalità da cause cardiovascolari N Engl J Med 2000; 342: 145.

54
Prevenzione primaria - HOT
Events/1000 pts-yrs Comparison RR(95%CI) Major Cardiovascular Events <90mmHg 24.4 90vs85 1.32( ) <85mmHg 18.6 85vs80 1.56( ) <80mmHg 11.9 90vs80 2.06( ) Cardiovascular mortality <90mmHg 11.1 90vs85 0.99( ) <85mmHg 11.2 85vs80 3.0( ) <80mmHg 3.7 90vs80 3.0( ) Lancet 1998; 351:
 Major Cardiovascular Events. <90mmHg vs ( ) <85mmHg vs ( ) <80mmHg vs ( ) Cardiovascular mortality. <90mmHg vs ( ) <85mmHg vs ( ) <80mmHg vs ( ) Lancet 1998; 351:")
55
Prevenzione primaria ASA 325 mg a giorni alterni vs placebo
Eventi cardiovascolari maggiori - 4% p=n.s. Infarto miocardico - 44% p< Infarto miocardico fatale - 64% p=0.07 Stroke P=n.s. Stroke emorragico RR 2.14 p=0.06 Physicians’ Health Study, N Engl J Med 1989; 321:

56
Prevenzione primaria ASA 75 mg / die vs placebo
Eventi cardiovascolari maggiori -15% p=0.002 Infarto miocardico -36% p=0.002 Stroke P=n.s. Sanguinamenti maggiori P=n.s. Sanguinamenti minori 2 volte più frequenti HOT, Lancet 1998; 351:

58
Delay in Initiation of Reperfusion Therapy
Treatment Delayed is Treatment Denied Symptom Recognition Call to Medical System PreHospital ED Cath Lab Increasing Loss of Myocytes Evidence exists that expeditious restoration of flow in the obstructed infarct artery after the onset of symptoms in patients with STEMI is the key determinent of short- and long-term outcomes regardless of whether reperfusion is accomplished by fibrinolysis or PCI. Efforts should be made to shorten the time from recognition of symptoms by the patient to contact with the medical system. Delay in Initiation of Reperfusion Therapy

59
Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Boersma E, Maas AC, Deckers JW, Simoons ML. Lancet Sep 21;348(9030):771-5.
:")
60
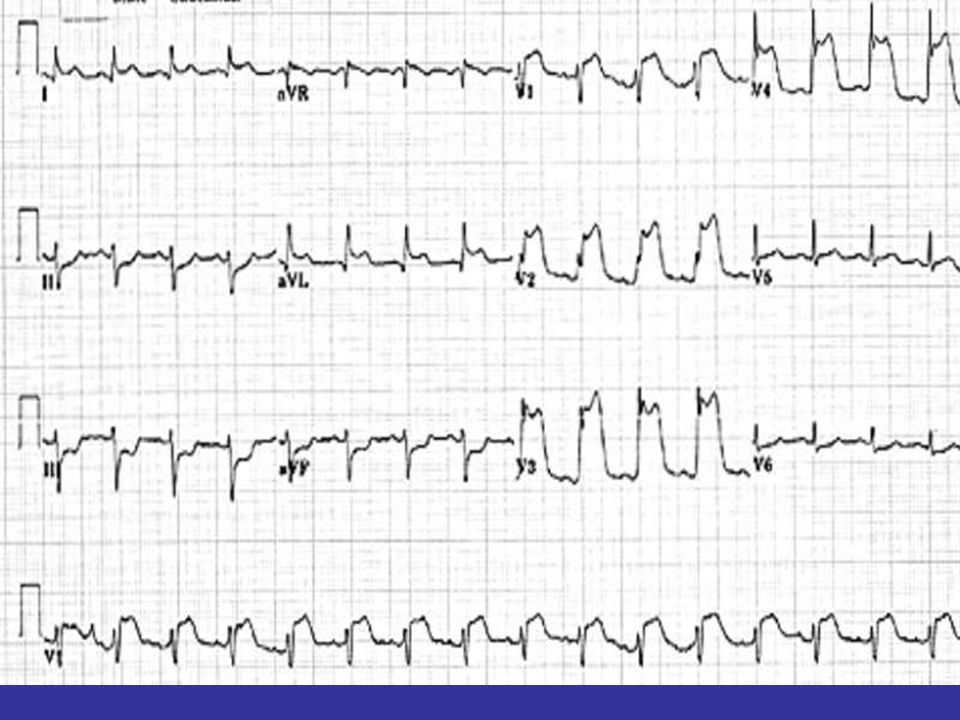
Post stent Pre angioplastica

Presentazioni simili







 NONLIPID RISK FACTORS>")





>")

 17 Ottobre 2009 DOPPIA ANTIAGGREGAZIONE PIASTRINICA.>")



