Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
COMPLICANZE

2
CAUSE DI MORTE NEGLI U.S.A.
100 200 300 400 Morti / anno (migliaia) È evidente che un tale aumento di morbilità per alcune neoplasie e per patologie che a loro volta inducono importanti alterazioni cardiovascolari determina inevitabilmente un aumento di mortalità. Uso di droghe Incidenti stradali Armi da fuoco Alcool Infezioni Obesità Fumo McGinnis et al, JAMA, 1993
 È evidente che un tale aumento di morbilità per alcune neoplasie e per patologie che a loro volta inducono importanti alterazioni cardiovascolari determina inevitabilmente un aumento di mortalità. Uso di. droghe. Incidenti. stradali. Armi. da fuoco. Alcool. Infezioni. Obesità. Fumo. McGinnis et al, JAMA,")
3
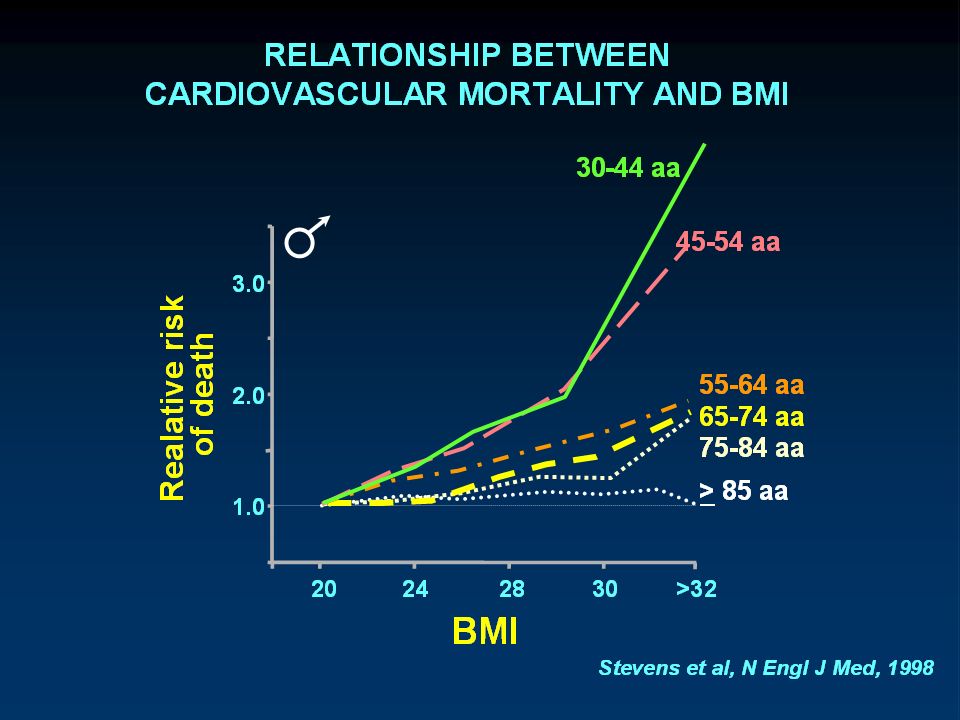
RELAZIONE TRA MORTALITÀ E BMI
0,0 0,5 1,0 1,5 2,0 2,5 Rischio relativo Mortalità Molto alto Molto basso Basso Moderato Alto Questa diapositiva mostra la relazione curvilinea tra mortalità e BMI. Le classi di rischio sono state ottenute da studi effettuati su popolazioni caucasiche e non è quindi certo che esse possano essere estendibili anche ad altre popolazioni. 20 25 30 35 40 BMI Bray, Clin Endocrinol Metab, 1999

4
RELATIONSHIP BETWEEN BMI AND THE RELATIVE RISK OF:
Type 2 Diabetes 1 2 3 4 5 6 Hypertension Cholelithiasis Realative risk Coronary heart disease Morbilità: dati epidemiologici. Nurses’ Health Study (Età: seguite per 18 anni) Come si può notare l’aumento del rischio ha inizio nell’ambito del sovrappeso; mentre per il diabete vi è un aumento lineare del rischio partendo da un BMI del tutto normale. 20 21 22 23 24 25 26 27 28 29 30 BMI Willet et al, N Engl J Med, 1999
 Come si può notare l’aumento del rischio ha inizio nell’ambito del sovrappeso; mentre per il diabete vi è un aumento lineare del rischio partendo da un BMI del tutto normale BMI. Willet et al, N Engl J Med,")
5
Body Mass Index - B M I (Kg/m2)
< = Sottopeso = Normopeso = Sovrappeso = Obesità classe I = Obesità classe II > 40 = Obesità classe III International Obesity Task Force

6
RELAZIONE TRA DECILI DI CIRONFERENZA VITA E BMI E RISCHIO RELATIVO DI DIABETE TIPO 2
RR Diabete tipo 2 Decili Circonferenza vita BMI L’importanza dell’obesità addominale come fattore di rischio per il diabete tipo 2 è stata confermata dall’ Health Professional Follow-up Study su soggetti, nei quali sono stati confrontati l’IMC , la CV e il rapporto V/F nel predire il diabete durante un follow up di 13 anni. I risultati di questo studio mostrano chiaramente che la CV ha una capacità predittiva superiore all’IMC e al rapporto V/F. Wang et al, Am J Clin Nutr, 81: , 2005

10
MORBILITÀ NELL’OBESITÀ
Sindrome Metabolica: Insulino-resistenza, diabete, dislipidemia, ipertensione; Malattie cardiovascolari Neoplasie Colelitiasi Artrosi Disordini psico-sociali Apparato respiratorio: Insufficienza restrittiva (grandi obesi); Apnee notturne (potenziale grave ipossia).
; Apnee notturne (potenziale grave ipossia).")
11
OBESITÀ E RISCHIO CARDIOVASCOLARE
Ipertrofia ventricolo sn. Morte improvvisa Ipertensione Cause dirette Sindrome Metabolica: Insulino-resistenza, diabete, dislipidemia, ipertensione; Cause indirette

12
CAUSE DIRETTE Ipertrofia del ventricolo sinistro Morte improvvisa
- Volemia (sodio-ritenzione, attivaz. simpatica, PRA) - Gittata sistolica - Postcarico Morte improvvisa - Aritmie (Ipertrofia ventr sin; dilataz. atrio sin; infiltrazione grassa del sistema di conduzione) - Q-T - Apnee notturne
 - Gittata sistolica. - Postcarico. Morte improvvisa. - Aritmie (Ipertrofia ventr sin; dilataz. atrio sin; infiltrazione grassa del sistema di conduzione) - Q-T. - Apnee notturne.")
13
CAUSE INDIRETTE Sn. Metabolica
(oppure Sn. da insulino-resistenza o Sn. X) • Insulino-resistenza • Iperinsulinemia • Diabete tipo 2 o IGT o IFG • Ipertensione • HDL • Trigliceridi • Apo B • LDL piccole e dense • Fibrinogeno • PAI-1 • IL-6 e PCR • Disfunzione endoteliale
 • Insulino-resistenza. • Iperinsulinemia. • Diabete tipo 2 o IGT o IFG. • Ipertensione. • HDL. • Trigliceridi. • Apo B. • LDL piccole e dense. • Fibrinogeno. • PAI-1. • IL-6 e PCR. • Disfunzione endoteliale.")
14
G.B. Morgagni Around 1750, Joannes Baptista Morgagni clearly described increased intraabdominal and mediastinal fat accumulation in android obesity. Remarkably, he also recognized the association between visceral obesity, hypertension, hyperuricemia, atherosclerosis, and obstructive sleep apnea syndrome.

15
In 1947, Jean Vague “rediscovered” the importance of the “android” obesity phenotype and its association with diabetes, atherosclerosis, gout, and uric-acid calculous disease. Vague J. La différenciacion sexuelle, facteur déterminant des formes de l'obésité. Presse Med;30:339-40, 1947 Vague J. The degree of masculine differentiation of obesities: a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am J Clin Nutr.;4:20–34, 1956

16
Overweight, Obesity, and Mortality in a Large Prospective
Cohort of Persons 50 to 71 Years Old , aa, 10 yrs Adams et al, NEJM, 2006

17
The IOWA Woman’s Health Study
ASSOCIATION OF GENERAL AND ABDOMINAL OBESITY WITH MULTIPLE HEALTH OUTCOMES IN OLDER WOMAN The IOWA Woman’s Health Study Uterine Cancer 31.700 55-69 aa Folsom AF et al, Arch Internal Med, 2000

18
RELAZIONE TRA DECILI DI CIRONFERENZA VITA E BMI E RISCHIO RELATIVO DI DIABETE TIPO 2
RR Diabete tipo 2 Decili Circonferenza vita BMI L’importanza dell’obesità addominale come fattore di rischio per il diabete tipo 2 è stata confermata dall’ Health Professional Follow-up Study su soggetti, nei quali sono stati confrontati l’IMC , la CV e il rapporto V/F nel predire il diabete durante un follow up di 13 anni. I risultati di questo studio mostrano chiaramente che la CV ha una capacità predittiva superiore all’IMC e al rapporto V/F. Wang et al, Am J Clin Nutr, 81: , 2005

19
INTERNATIONAL DAY FOR THE EVALUATION OF ABDOMINAL OBESITY (IDEA)
A Study of Waist Circumference, Cardiovascular Disease, and Diabetes Mellitus in Primary Care Patients in 63 Countries Frequency (%) CVD DIABETES Frequency (%) Waist Circunference (cm) Balkau B et al, Circulation, 2007
 CVD. DIABETES. Frequency (%) Waist Circunference (cm) Balkau B et al, Circulation,")
20
LOWER-BODY ADIPOSITY AND METABOLIC PROTECTION IN POSTMENOPAUSAL WOMEN
Triglycerides (mg/dl) In 95 donne sovrappeso in postmenopausa l’entità del grasso viscerale e di quello sottocutaneo delle gambe è stato messo in relazione a vari parametri metabolici: non solo il grasso delle gambe non correlava con nessuno dei parametri metabolici, ma anzi si è osservata la tendenza ad una correlazione inversa con le concentrazioni plasmatiche di trigliceridi, come se maggiori riserve di grasso sottocutaneo a livello delle coscie fossero protettive. Visceral Fat Leg Fat Van Pelt et al, J Clin Endocrinol Metab, 90:4573–4578, 2005
 In 95 donne sovrappeso in postmenopausa l’entità del grasso viscerale e di quello sottocutaneo delle gambe è stato messo in relazione a vari parametri metabolici: non solo il grasso delle gambe non correlava con nessuno dei parametri metabolici, ma anzi si è osservata la tendenza ad una correlazione inversa con le concentrazioni plasmatiche di trigliceridi, come se maggiori riserve di grasso sottocutaneo a livello delle coscie fossero protettive. Visceral Fat. Leg Fat. Van Pelt et al, J Clin Endocrinol Metab, 90:4573–4578,")
21
Low sc thigh fat is a risk factor for unfavourable glucose and lipid levels
The Health ABC Study Fasting glucose (mmol/l) Health, Aging, and Body Composition (Health ABC) Study. Anthropometric measurements and computed tomography of the abdomen and of the thigh were performed for all participants of the Health, Aging and Body Composition Study, who were aged 70–79 years. Fasting glucose, triglycerides and HDL-cholesterol, and 2-h postload glucose were determined. Larger subcutaneous thigh fat is independently associated with more favourable glucose (in men) and lipid levels (in both sexes) after accounting for abdominal fat depots, which are associated with unfavourable glucose and lipid levels. Anthropometric measures reflectdifferent fat depots at different levels of BMI at the abdomen, and reflect both fat and lean tissue at the thigh. These results emphasise the importance of accurate measures of regional body composition when investigating potential health risks. SC thigh Fat tertiles Visceral Fat tertiles 3.000, aa Snijder et al, Diabetologia, 2005
 Health, Aging, and Body Composition (Health ABC) Study. Anthropometric measurements and computed tomography of the abdomen and of the thigh were performed for all participants of the Health, Aging and Body Composition Study, who were aged 70–79 years. Fasting glucose, triglycerides and HDL-cholesterol, and 2-h postload glucose were determined. Larger subcutaneous thigh fat is independently associated with more favourable glucose (in men) and lipid levels (in both sexes) after accounting for abdominal fat depots, which are associated with unfavourable glucose and lipid levels. Anthropometric measures reflectdifferent fat depots at different levels of BMI at the abdomen, and reflect both fat and lean tissue at the thigh. These results emphasise the importance of accurate measures of regional body composition when investigating potential health risks. SC thigh Fat. tertiles. Visceral Fat. tertiles , aa. Snijder et al, Diabetologia,")
22
PREVALENZA DI RISCHIO 10-y-CHD > 15% HEALTH SURVEY FOR ENGLAND
PER CLASSI DI BMI E WHR: HEALTH SURVEY FOR ENGLAND Prevalenza CHD % 3090 men in the Framingham study and 2571 men in the 1998 Health Survey for England (HSE) aged 35–74 y with no history of cardiovascular disease. Fig: Prevalence (%) of predicted 10-yCHD risk >15% according to WHR and BMI in men aged 35–74 y. Che la misura dell’accumulo di adipe a livello addominale e non il BMI rappresenti un fattore di rischio CV è stato di recente ben dimostrato dallo studio “Health Survey for England” (D16): circa 2500 soggetti con anamnesi negativa per malattie CV sono stati stratificati per BMI e per rapporto vita/fianchi ed è stata calcolata la prevalenza di soggetti con un rischio per CAD a 10 anni maggiore del 15% secondo le carte del rischio di Framingham. Ebbene, tra i pazienti con BMI < 23, quindi perfettamente normopeso, ma con accumulo di adipe a livello addominale (rapporto vita/fianchi > 1,0) il 48% aveva un rischio a 10 anni maggiore del 15%, mentre tra i soggetti obesi (BMI>30) ma con rapporto vita/fianchi di 0,85 la prevalenza era del 20%. Rapporto Vita/Fianchi BMI 3.000 Nanchahal et al, Int J Obes 29:317, 2005
 aged 35–74 y. with no history of cardiovascular disease. Fig: Prevalence (%) of predicted 10-yCHD risk >15% according to WHR and BMI in men aged 35–74 y. Che la misura dell’accumulo di adipe a livello addominale e non il BMI rappresenti un fattore di rischio CV è stato di recente ben dimostrato dallo studio Health Survey for England (D16): circa 2500 soggetti con anamnesi negativa per malattie CV sono stati stratificati per BMI e per rapporto vita/fianchi ed è stata calcolata la prevalenza di soggetti con un rischio per CAD a 10 anni maggiore del 15% secondo le carte del rischio di Framingham. Ebbene, tra i pazienti con BMI < 23, quindi perfettamente normopeso, ma con accumulo di adipe a livello addominale (rapporto vita/fianchi > 1,0) il 48% aveva un rischio a 10 anni maggiore del 15%, mentre tra i soggetti obesi (BMI>30) ma con rapporto vita/fianchi di 0,85 la prevalenza era del 20%. Rapporto. Vita/Fianchi. BMI Nanchahal et al, Int J Obes 29:317,")
23
Obesity and the risk of MI in 27000 participants from 52 countries: a case-control study
INTERHEART study AMI Figure : Association of BMI and waist-to-hip ratio with myocardial infarction risk Methods We did a standardised case-control study of acute myocardial infarction with participants in 52 countries ( cases and controls) representing several major ethnic groups. We assessed the relation between BMI, waist and hip circumferences, and waist-to-hip ratio to myocardial infarction overall and for each group. Interpretation Waist-to-hip ratio shows a graded and highly significant association with myocardial infarction risk worldwide. Redefinition of obesity based on waist-to-hip ratio instead of BMI increases the estimate of myocardial infarction attributable to obesity in most ethnic groups. BMI quintiles Waist-to-hip quintiles Yusuf S et al, Lancet, 366: , 2005
 representing several major ethnic groups. We assessed the relation between BMI, waist and hip circumferences, and waist-to-hip ratio to myocardial infarction overall and for each group. Interpretation Waist-to-hip ratio shows a graded and highly significant association with myocardial infarction risk worldwide. Redefinition of obesity based on waist-to-hip ratio instead of BMI increases the estimate of myocardial infarction attributable to obesity in most ethnic groups. BMI quintiles. Waist-to-hip quintiles. Yusuf S et al, Lancet, 366: ,")
24
Obesity and the risk of MI in 27000 participants from 52 countries: a case-control study
INTERHEART study AMI Figure: Risk of MI associated with increasing waist circumference and hip circumference Methods We did a standardised case-control study of acute myocardial infarction with participants in 52 countries ( cases and controls) representing several major ethnic groups. Consecutive cases of first myocardial infarction presenting within 24 h of symptom onset were eligible. We assessed the relation between BMI, waist and hip circumferences, and waist-to-hip ratio to myocardial infarction overall and for each group. Interpretation Waist-to-hip ratio shows a graded and highly significant association with myocardial infarction risk worldwide. Redefinition of obesity based on waist-to-hip ratio instead of BMI increases the estimate of myocardial infarction attributable to obesity in most ethnic groups. Waist quintiles Hip quintiles Yusuf S et al, Lancet, 366: , 2005
 representing several major ethnic groups. Consecutive cases of first myocardial infarction presenting within 24 h of symptom onset were eligible. We assessed the relation between BMI, waist and hip circumferences, and waist-to-hip ratio to myocardial infarction overall and for each group. Interpretation Waist-to-hip ratio shows a graded and highly significant association with myocardial infarction risk worldwide. Redefinition of obesity based on waist-to-hip ratio instead of BMI increases the estimate of myocardial infarction attributable to obesity in most ethnic groups. Waist quintiles. Hip quintiles. Yusuf S et al, Lancet, 366: ,")
25
PREVALENZA DI OBESITÀ ADDOMINALE NELLA S. METABOLICA (NCEP)
NHANES 1999–2002 (3.601, > 20 aa) “STUDIO LINOSA”: (364, > 18 aa) SM NCEP 21.4% Bellia et al, Diabetes (ADA) 2004 Ford ES, Diabetes Care 2005
 STUDIO LINOSA : (364, > 18 aa) SM. NCEP. 21.4% Bellia et al, Diabetes (ADA) Ford ES, Diabetes Care")
26
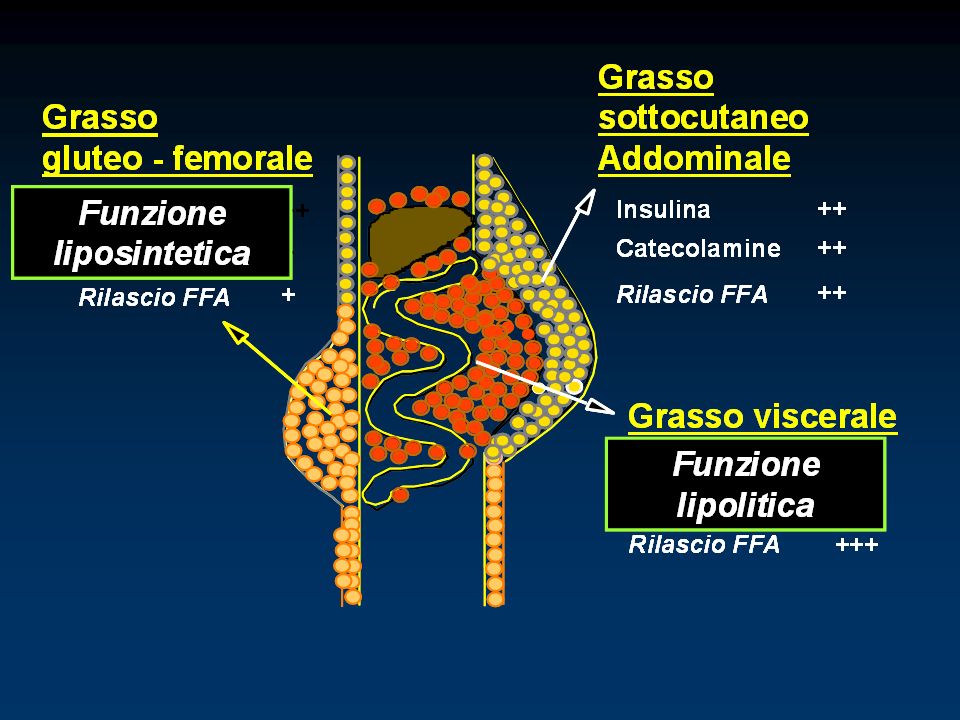
centripeta, androide periferica, ginoide
DISTRIBUZIONE DEI DEPOSITI DI GRASSO centripeta, androide periferica, ginoide

28
VISCERAL vs SUBCUTANEOUS FAT
insulin antilipolytic effect. expression of cortiocosteroids receptors. DEX-induced LPL stimulation. expression of androgen receptors. High FFA portal flux increases hepatic glucose production and VLDL synthesis. cathecolamines lipolytic effect. TZD effects on preadipocytes.

29
PREADIPOCYTE ADIPOCYTE Energy Homeostasis LPL HSL Innate Immune System
Leptin Adiponectin Resistin Visfatin 1 Glicop. SAA3 PTX Innate Immune System TNF IL-6 Acute Phase Reactant Response VEGF Angiotensin II Vascular Remodeling LPL HSL Lipoprotein Metabolism Fibrinolysis PAI-1 ADIPOCYTE PREADIPOCYTE

30
Properties of key adipokines
Adiponectin in IAA Anti-atherogenic/antidiabetic: foam cells vascular remodelling insulin sensitivity hepatic glucose output IL-6 in IAA Pro-atherogenic/pro-diabetic: vascular inflammation insulin signalling TNFa insulin sensitivity in adipocytes (paracrine) PAI-1 Pro-atherogenic: atherothrombotic risk Properties of key adipokines Here we examine key adipocyte-derived bioactive substances (‘adipokines’) in more detail. Adiponectin exerts a number of protective actions in the vasculature, including inhibition of foam cell formation and vascular remodelling, both important steps in the formation of an atherosclerotic plaque. This hormone also improves insulin sensitivity and opposes the development of hyperglycaemia, and is therefore antidiabetic as well as anti-atherosclerotic in nature. IL-6 is a systemic inflammatory hormone that exerts adverse, pro-atherogenic effects in the vasculature. IL-6 also exacerbates insulin resistance and is therefore both pro-atherogenic and pro-diabetic. TNFa is a paracrine regulator in adipocytes. TNFa-induced reductions in insulin sensitivity in adipocytes are partly responsible for the increased free fatty acid production and hypertriglyceridaemia characteristic of abdominal obesity. Increased PAI-1 secretion by intra-abdominal adipocytes shifts the balance of fibrinolysis towards a procoagulant state, increasing the risk of a morbid thromboembolic event. Marette A. Mediators of cytokine-induced insulin resistance in obesity and other inflammatory settings. Curr Opin Clin Nutr Metab Care 2002;5: IAA: intra-abdominal adiposity Marette 2002
 PAI-1. Pro-atherogenic: atherothrombotic risk. Properties of key adipokines. Here we examine key adipocyte-derived bioactive substances (‘adipokines’) in more detail. Adiponectin exerts a number of protective actions in the vasculature, including inhibition of foam cell formation and vascular remodelling, both important steps in the formation of an atherosclerotic plaque. This hormone also improves insulin sensitivity and opposes the development of hyperglycaemia, and is therefore antidiabetic as well as anti-atherosclerotic in nature. IL-6 is a systemic inflammatory hormone that exerts adverse, pro-atherogenic effects in the vasculature. IL-6 also exacerbates insulin resistance and is therefore both pro-atherogenic and pro-diabetic. TNFa is a paracrine regulator in adipocytes. TNFa-induced reductions in insulin sensitivity in adipocytes are partly responsible for the increased free fatty acid production and hypertriglyceridaemia characteristic of abdominal obesity. Increased PAI-1 secretion by intra-abdominal adipocytes shifts the balance of fibrinolysis towards a procoagulant state, increasing the risk of a morbid thromboembolic event. Marette A. Mediators of cytokine-induced insulin resistance in obesity and other inflammatory settings. Curr Opin Clin Nutr Metab Care 2002;5: IAA: intra-abdominal adiposity. Marette")
31
Visceral Adip Tissue (VAT) Subcutaneous Adip Tissue (SAT)
Adipokine PAI-1 IL-6 Leptin Adiponectin TNF-a Angiotensinogen Resistin Visceral Adip Tissue (VAT) Vs Subcutaneous Adip Tissue (SAT) VAT> SAT VAT > SAT SAT > VAT ?
 Vs. Subcutaneous Adip Tissue (SAT) VAT> SAT. VAT > SAT. SAT > VAT.")
32
viscerale e sottocutaneo rispondono in modo diverso (espressione di geni)
resistina leptina angiot.-geno adiponectina 50 6 8 8 40 6 6 4 30 4 4 20 2 2 2 10 SC visc. SC visc. SC visc. SC visc. PAI-1 IL-6 IL-10 TNF-a 8 5 6 4 4 6 3 4 3 4 2 2 2 2 1 1 SC visc. SC visc. SC visc. SC visc. digiuno iperglicemia iperinsulinemia Einstein FH et al: Diabetes 54:672, 2005

33
INS. RES.

34
Removal of Visceral Fat Prevents Insulin Resistance of Aging
? * M (mg/kg/min) * In ratti adulti (20 mesi) è stato rimosso chirurgicamente il grasso viscerale (no VF) ed è stata misurata la sensibilità insulinica e la produzione epatica di glucosio paragonandola a ratti giovani (2 mesi), a ratti di controllo (SO), a ratti nei quali era stata rimossa la stessa quantità di grasso sottocutaneo (no SC) ed a ratti in regime di restrizione calorica (CR): il declino fisiologico con l’aumentare dell’età dei due parametri analizzati è stato reso completamente reversibile dalla rimozione del grasso viscerale, in misura lievemente migliore di quanto ottenuto dalla restrizione calorica. Nessun effetto è stato invece osservato nei ratti “no SC”. HGP (mg/kg/min) Gabriely et al, Diabetes, 51: , 2002
 * In ratti adulti (20 mesi) è stato rimosso chirurgicamente il grasso viscerale (no VF) ed è stata misurata la sensibilità insulinica e la produzione epatica di glucosio paragonandola a ratti giovani (2 mesi), a ratti di controllo (SO), a ratti nei quali era stata rimossa la stessa quantità di grasso sottocutaneo (no SC) ed a ratti in regime di restrizione calorica (CR): il declino fisiologico con l’aumentare dell’età dei due parametri analizzati è stato reso completamente reversibile dalla rimozione del grasso viscerale, in misura lievemente migliore di quanto ottenuto dalla restrizione calorica. Nessun effetto è stato invece osservato nei ratti no SC . HGP. (mg/kg/min) Gabriely et al, Diabetes, 51: ,")
35
EFFETTI DELLA RIMOZIONE DI TESSUTO ADIPOSO SOTTOCUTANEO MEDIANTE LIPOSUZIONE
Prima Dopo 36% Nessun effetto su: Sensibilità insulinica Pressione arteriosa Glicemia Colesterolo tot. E HDL Trigliceridi FFA Leptina Adiponectina TNFα IL-6 PCR In 15 pazienti obese la rimozione mediante liposuzione di una media del 36% del volume di tessuto adiposo sottocutaneo non ha indotto alcun miglioramento della sensibilità insulinica e di nessuno dei parametri metabolici classici e delle concentrazioni plasmatiche delle principali adipochine. Klein et al, N Engl J Med, 350: , 2004

36
LIPODISTROFIE PARZIALI Mandibuloacral dysplasia
AF BMI: 14.3 Circ. vita: 68 cm Massa grassa: 15.4% BMI: 21.2 Circ. vita: 91 cm Massa grassa: 24.8% WP NORMALE Sbraccia et al, Diabetes (ADA) 2004
")
37
lipotoxicity: too fat in the wrong tissue
spill-over atherosclerosis insulin-resist. steatosis diabetes

38
il deposito di trigliceridi determina insulino-resistenza
TG nel muscolo TG nel fegato 0.1 0.2 0.3 0.05 0.10 0.15 u.a. giovani anziani giovani anziani Cree MG et al.: J Clin Endocrinol Metab 89:3864, 2004

39
INFIAMMAZIONE E DIABETE TIPO 2
NIDDM as a Disease of the Innate Immune System: Association of Acute-phase Reactants and Interleukin-6 with Metabolic Syndrome X. Pickup JC et al, Diabetologia 40:1286 –1292, 1997 Insulin Resistance And Adiposity Correlate With Acute-phase Reaction and Soluble Cell Adhesion Molecules in Type 2 Diabetes. Leinonen E et al, Atherosclerosis 166:387–394, 2003

40
INFIAMMAZIONE E DT2: STUDI PROSPETTICI
High White Blood Cell Count is Associated With a Worsening of Insulin Sensitivity and Predicts the Development of Type 2 Diabetes. Vozarova B et al, Diabetes 51:455– 461, 2002 The Relation of Markers Of Inflammation To The Development of Glucose Disorders in the Elderly: The Cardiovascular Health Study. Barzilay JI et al, Diabetes 50:2384 –2389, 2001 Low-grade Systemic Inflammation and the Development of Type 2 Diabetes: The Atherosclerosis Risk In Communities Study. Duncan BB et al, Diabetes 52:1799 –1805, 2003

41
BMI Infiammatori Markers PCR IL-6 Fibrinogeno 1-glicoproteina acida
Kern et al, Am J Physiol Endocrinol Metab. 2001 Cottam et al, Obes Surg. 2004 Yudkin et al, Atherosclerosis. 2000 Berg & Sherer, Circulation 2005

42
Impact of Weight Loss on Inflammatory Proteins and Their
Association With the Insulin Resistance Syndrome in Morbidly Obese Patients CRP IL-6 TNF Kopp et al, Arterioscler Thromb Vasc Biol.2003

43
CRP Intensive Lifestyle Intervention or Metformin on
Inflammation and Coagulation in Participants With Impaired Glucose Tolerance The Diabetes Prevention Program Research Group CRP Diabetes 2005

46
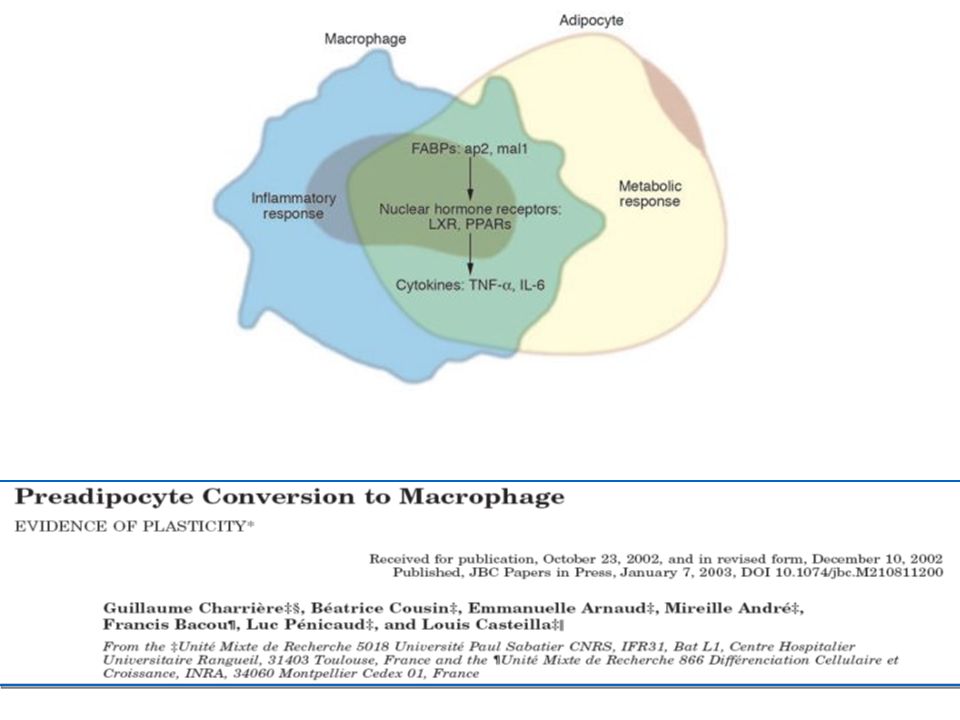
Xu et al, J Clin Invest 2003 Weisberg et al, J Clin Invest 2003

Presentazioni simili



 NONLIPID RISK FACTORS>")






 STEATOSI CIRROSI (8-25%) HCC.>")
 Guidelines May 2001 Ipercolesterolemie famigliari Ipercolesterolemie e rischio cardio vascolare globale.>")

 N. Pazienti in Dialisi (2002: 308.910)>")



 sottoposto a CABG.>")


