Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
MALATTIA METASTATICA ORMONOSENSIBILE
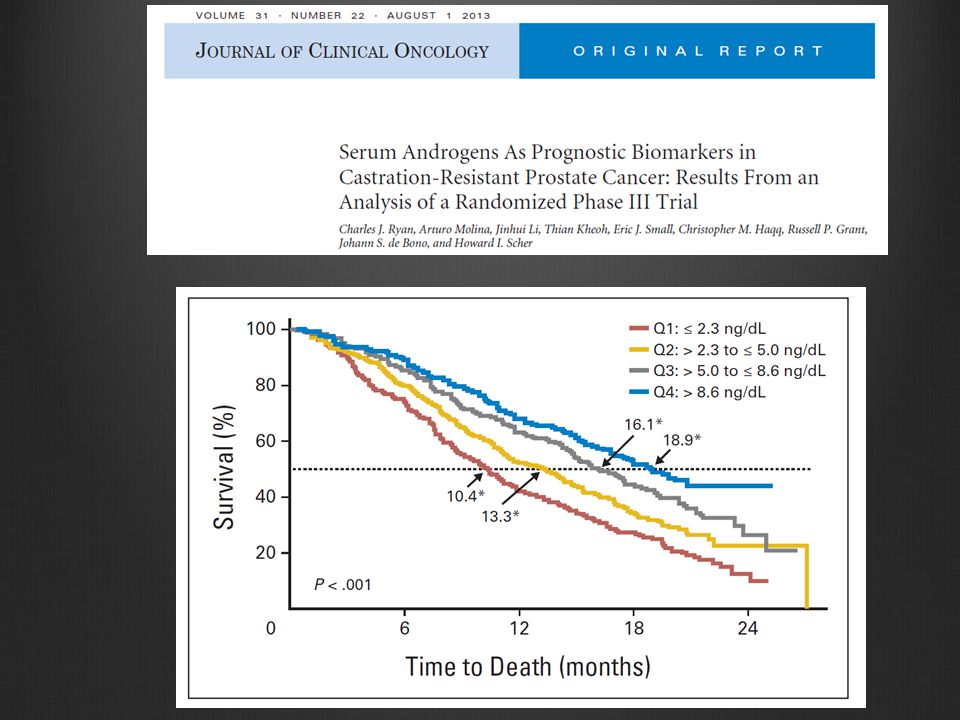
Nel paziente in trattamento ormonale c'è una relazione fra livelli circolanti di testosterone raggiunti e risposta alla terapia? 1

2
MALATTIA METASTATICA ORMONOSENSIBILE
Nel paziente in trattamento ormonale c'è una relazione fra livelli circolanti di testosterone raggiunti e risposta alla terapia? 2

3
BJU Int. 2010;105(5):648-51
:")
4
J Urol 178: 1290-1295, 2007 <20 ng/dl <32 ng/dl 20-50 ng/dl

5
Non metastatic patients Metastatic patients
Clin Genitourin Cancer 3: , 2013 Non metastatic patients Metastatic patients

6
Overall survival from PSA progression
<0.30 ng/ml >=0.30 ng/ml

7
Prognostic role = Surrogacy

8
PRENTICE’s criteria Treatment effect on the surrogate
Treatment effect on the primary Correlation between primary and surrogate Treatment effect on the primary disappears when the surrogate is adjusted for

9
Fig 1. Kaplan-Meier estimates of overall survival in TAX327 according to >= 30% prostate-specific antigen (PSA) decline status within first 3 months of treatment initiation Armstrong, A. J. et al. J Clin Oncol; 25:

10
PSA as a surrogate parameter of docetaxel efficacy SWOG study
P value HR 0.76 ( ) Univariate analysis docetaxel /E 0.052 Vs mitox/P HR 0.43 ( ) PSA decline >30% <0.001 Vs no decline Multivariate analysis HR 0.86 ( ) Docetaxel/E 0.16 Vs mitox/P 0.25 0.50 0.75 1 1.25 Hazard ratio (HR) and (95% CI) Proportion of Treatment effect Esplained (PTE): 1 (0.73-1) Patrylack DP et al JNCI 98: , 2006.
 Univariate. analysis. docetaxel /E Vs mitox/P. HR 0.43 ( ) PSA decline >30% < Vs no decline. Multivariate. analysis. HR 0.86 ( ) Docetaxel/E Vs mitox/P Hazard ratio (HR) and (95% CI) Proportion of Treatment effect Esplained (PTE): 1 (0.73-1) Patrylack DP et al JNCI 98: ,")
11
J Clin Endocrinol Metab 95: 4542–4548, 2010
Mass spectrometry as reference method for assessment of circulating testosterone in lower range

13
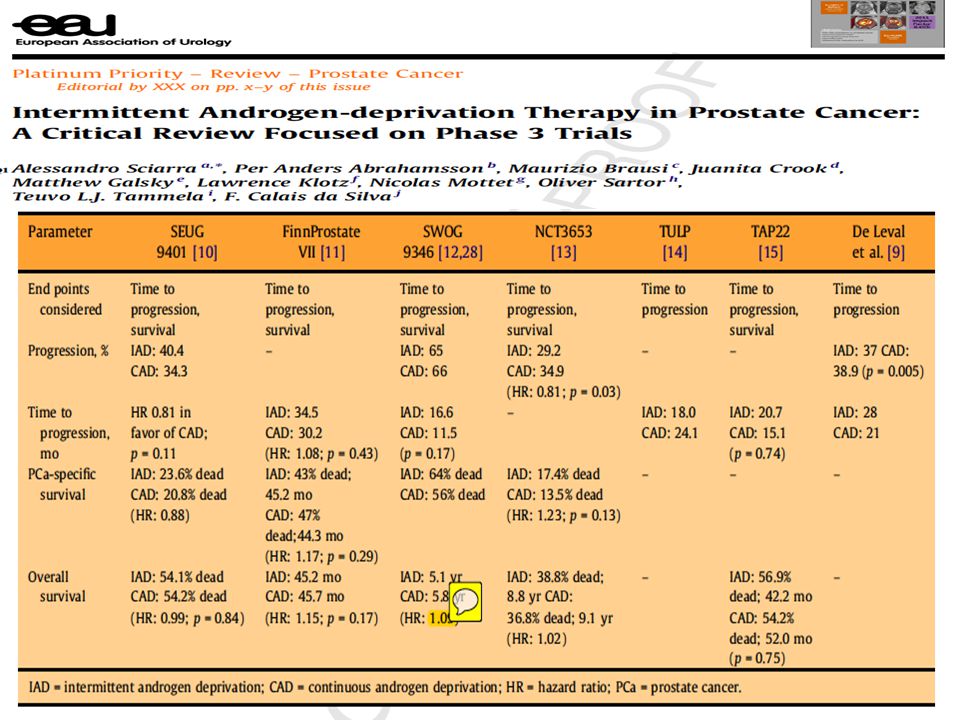
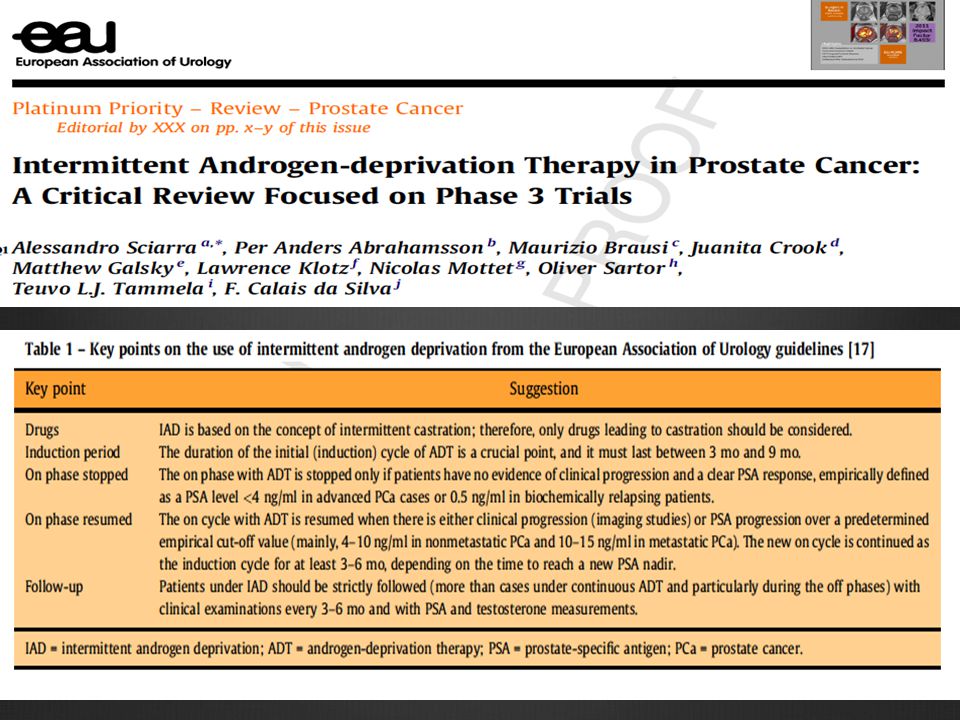
La terapia intermittente IAD: quali farmaci,
MALATTIA METASTATICA ORMONOSENSIBILE La terapia intermittente IAD: quali farmaci, quali indicazioni e quali vantaggi ? 13

15
Conclusion There is fair evidence to recommend use of IAD instead of CAD for the treatment of men with relapsing, locally advanced, or metastatic prostate cancer who achieve a good initial response to androgen deprivation. This recommendation is based on evidence against superiority of either strategy for time-to-event outcomes and substantial decrease with IAD in exposure to androgen deprivation, resulting in less cost, inconvenience, and potential toxicity.

16
Overall survival Time to progression Cancer specific survival

18
LHRH-A + antiandrogeni? Quali indicazioni
Quali farmaci LHRH-A + antiandrogeni? Quali indicazioni Paziente asintomatico con incremento di PSA specie se in assenza di metastasi Quali vantaggi Migliore tollerabilita? Minori costi Durata del periodo off come fattore prognostico aggiuntivo

19
Confronto LHRH analoghi ed antagonisti:
MALATTIA METASTATICA ORMONOSENSIBILE Confronto LHRH analoghi ed antagonisti: chi e’ il vincitore ? O esistono diverse indicazioni e sequenzialita ? 19

20
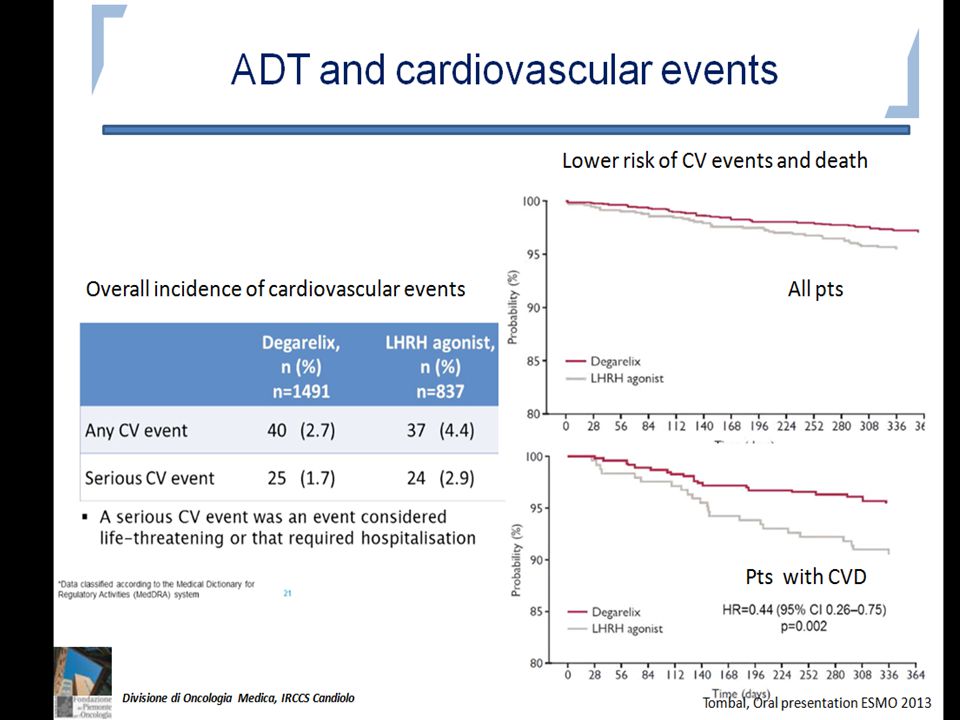
GNRH antagonists: Advantages
immediate reduction of serum testosterone - 72 h: 96% <0.5 ng/ml absence of testosterone initial flare up rapid reduction in PSA levels reduction in prostate volume already at 30 days reduction and stability on FSH limited half-life (10 days approximately)
")
21
Klotz L, Boccon-Gibod L, Shore ND, et al.
The efficacy and safety of degarelix: a 12-month, comparative, randomized, open-label, parallel-group phase III study in patients with prostate cancer. BJU Int 2008;102:1531–8 Primary aim: to demonstrate the non inferiority of degarelix versus leuprolide for the primary end point (probability of patients having testosterone 0.5 ng/ml at each monthly measurement for 1 yr)
")
22
Stratificando i pz in base a valore PSA iniziale, in quelli con PSA > 20, rischio progressione PSA maggiore con leuprolide che con degarelix. Ugualmnete , nei metastatici, PSA progressione maggiore con leuprolide che con degarelix. PSA progressione definita come aumento > 50% e valori superiori 5 ng/ml. Adesso si definisce come aumento 25% e valori superiori a 2.0 ng/ml.

23
FSH

25
Clin Oncol 2013 in press

26
Degarelix non inferiore in termini di
efficacia rispetto a Leuprolide + antiandrogeno Potenzialità di Degarelix In pazienti con malattia ossea estesa In pazienti con LUTS

27
Esiste ancora un ruolo per gli estrogeni ?
MALATTIA METASTATICA ORMONOSENSIBILE Esiste ancora un ruolo per gli estrogeni ? 27

28
Mechanisms of action of DES
Reduction of luteinizing hormone, testosterone and androgenic steroid levels1 Inhibition of telomerase activity2 direct binding of the androgen receptor (AR)3 Suppression of b-tubulin isotypes4 1Bosset PO et al BJU Int 2012; 110: E826–E829 2Geier R et al Prostate 2012; 70(12): 1307–1312. 3Wang H et al Asian J Androl 2010; 12(4): 535–547. 4Montgomery RB, et al: Prostate 2005; 65: 141–150.
3. Suppression of b-tubulin isotypes4. 1Bosset PO et al BJU Int 2012; 110: E826–E829. 2Geier R et al Prostate 2012; 70(12): 1307– Wang H et al Asian J Androl 2010; 12(4): 535–547. 4Montgomery RB, et al: Prostate 2005; 65: 141–150.")
29
BJC: 2013; 109:

30
Lancet Oncol 2007; 8: 994–1000

31
Quale follow-up nel paziente sottoposto ad ormonoterapia ?
MALATTIA METASTATICA ORMONOSENSIBILE Quale follow-up nel paziente sottoposto ad ormonoterapia ? 31

32
Main objectives of following-up during ADT
• monitor the response to treatment; • ensure compliance with treatment; • detect potential complications of endocrine therapy; • guide the modalities of palliative symptomatic treatment at the time of CRPC EAU guidelines 2013

33
Prognostic role of serum PSA levels
Patients with the lowest absolute value of serum PSA (< 0.2 ng/mL) have been shown to have the best survival compared to patients with a value of ng/mL or > 4.0 ng/mL 1 The PSA response in patients treated with hormonal therapy, following a rising PSA after treatments with curative intent (radical prostatectomy, radiation therapy) correlates with the best survival 2,3 1 Hussain M, et al J Clin Oncol 2006; 24(24): 2,D’Amico AV et al J Natl Cancer Inst 2004 ; 96 (7) : 3 Stewart AJ et al J Clin Oncol 2005; 23 (27):
 have been shown to have the best survival. compared to patients with a value of ng/mL or > 4.0 ng/mL 1. The PSA response in patients treated with hormonal therapy, following a rising PSA after treatments with curative intent. (radical prostatectomy, radiation therapy) correlates with the. best survival 2,3. 1 Hussain M, et al J Clin Oncol 2006; 24(24): ,D’Amico AV et al J Natl Cancer Inst 2004 ; 96 (7) : Stewart AJ et al J Clin Oncol 2005; 23 (27):")
34
Biochemistry: hemocrome, liver function tests, testosterone,
Vitamin D Monitoring metabolic complications

35
Imaging techniques Bone scan, ultrasonography. CT (?) on the basis of PSA changes and or clinics Dexa scan

Presentazioni simili