Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
I TUMORI VESCICALI

7
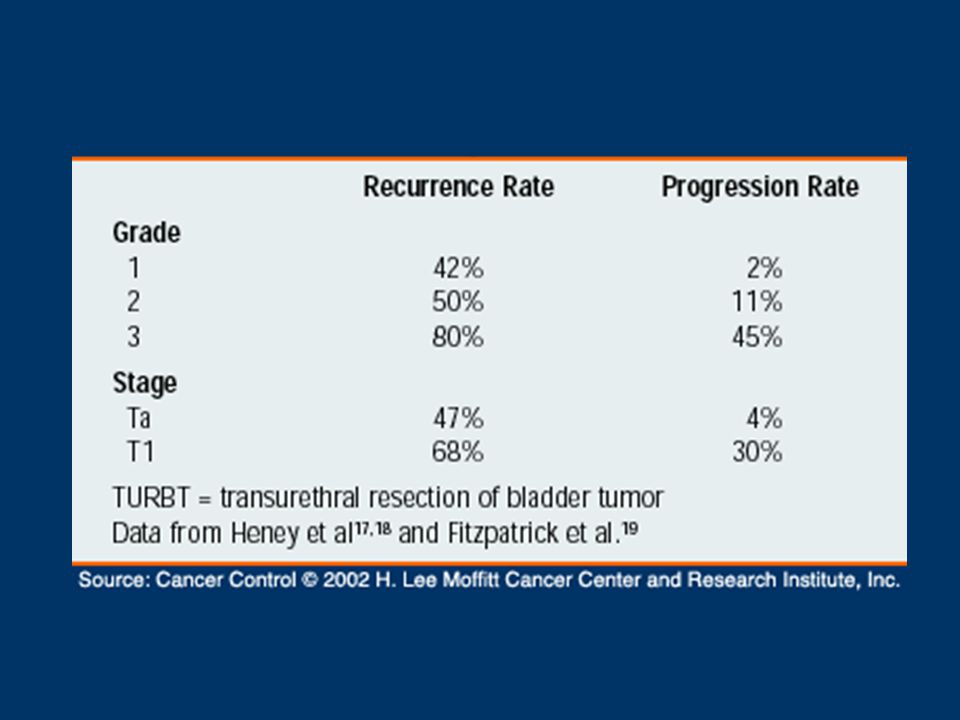
ANATOMIA PATOLOGICA Stadiazione
70 – 85 % 15 – 30 %

9
CLINICA Ematuria In 90% dei Pz con CaV Microscopica o macroscopica
Non correlata con stadio, grado, CaV Aspecifica: Litiasi, Flogosi, Nefropatie, RCC 5% dei Pz >50aa con microematuria ha CaV (10% se presenti altri sintomi [Es. irritativi]) “Any degree of haematuria, requires evaluation for bladder cancer, even if another potential cause of haematuria is found. [EAU Guidelines]
 Any degree of haematuria, requires evaluation for bladder cancer, even if another potential cause of haematuria is found. [EAU Guidelines]")
10
CLINICA Altri sintomi PRECOCI
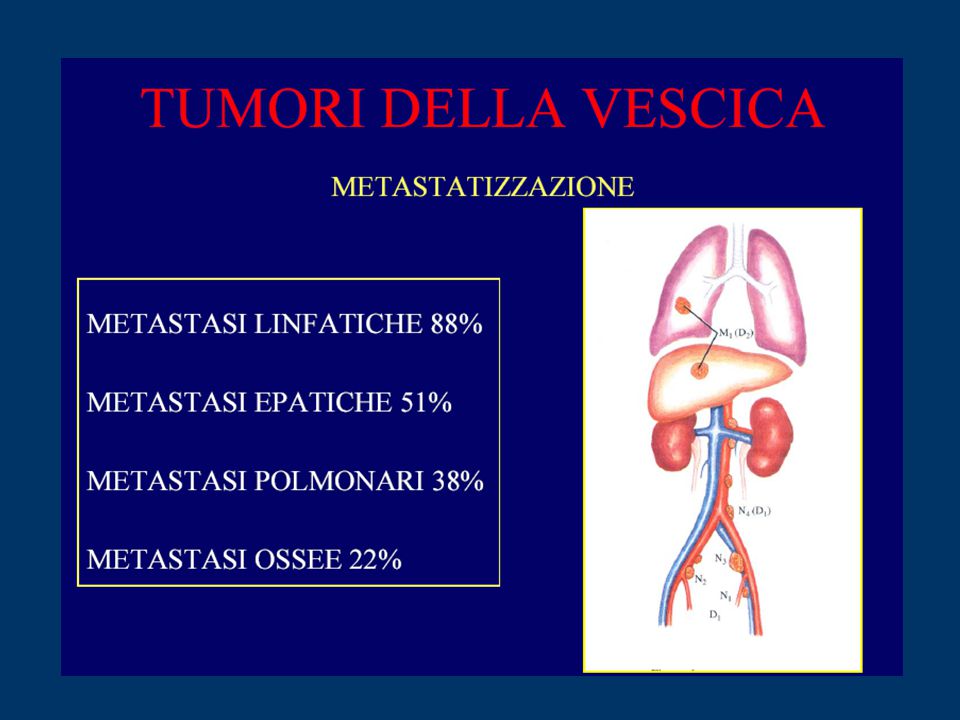
S. Irritativi minzionali (urgenza, frequenza) Disuria (raro) TARDIVI Idronefrosi (Ostruzione del meato ureterale) Dolore al fianco Dolore osseo (Metastasi ossee) Coliche addominali (Metastasi retroperit.) Astenia e perdita di peso
 Disuria (raro) TARDIVI. Idronefrosi (Ostruzione del meato ureterale) Dolore al fianco. Dolore osseo (Metastasi ossee) Coliche addominali (Metastasi retroperit.) Astenia e perdita di peso.")
13
ITER DIAGNOSTICO CISTOSCOPIA ESAME OBIETTIVO Addome, Pelvi
Retto, Vagina CISTOSCOPIA

14
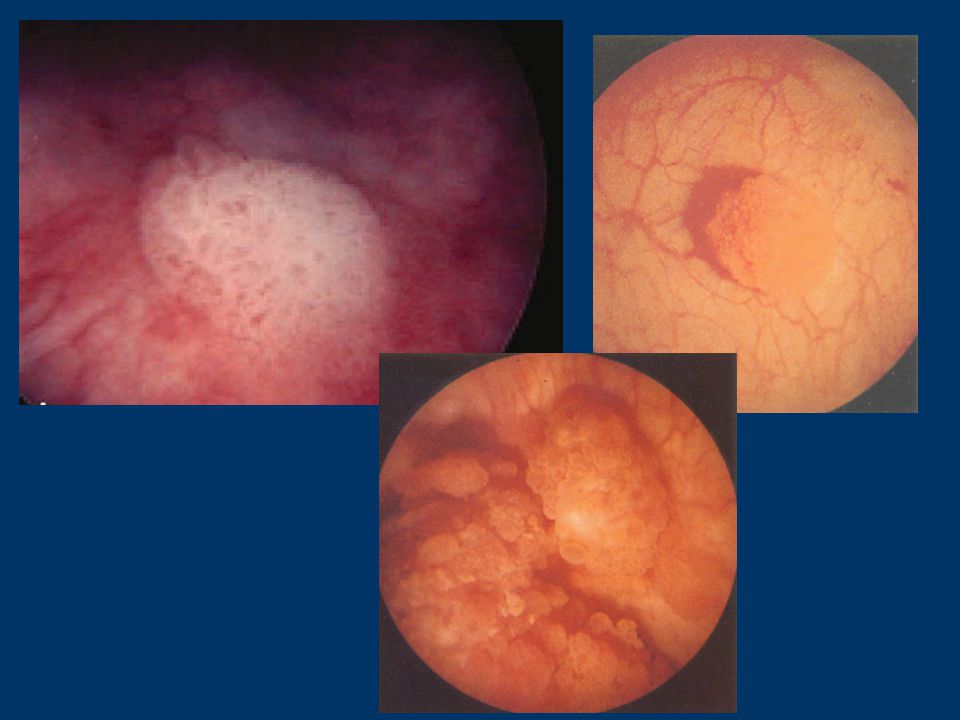
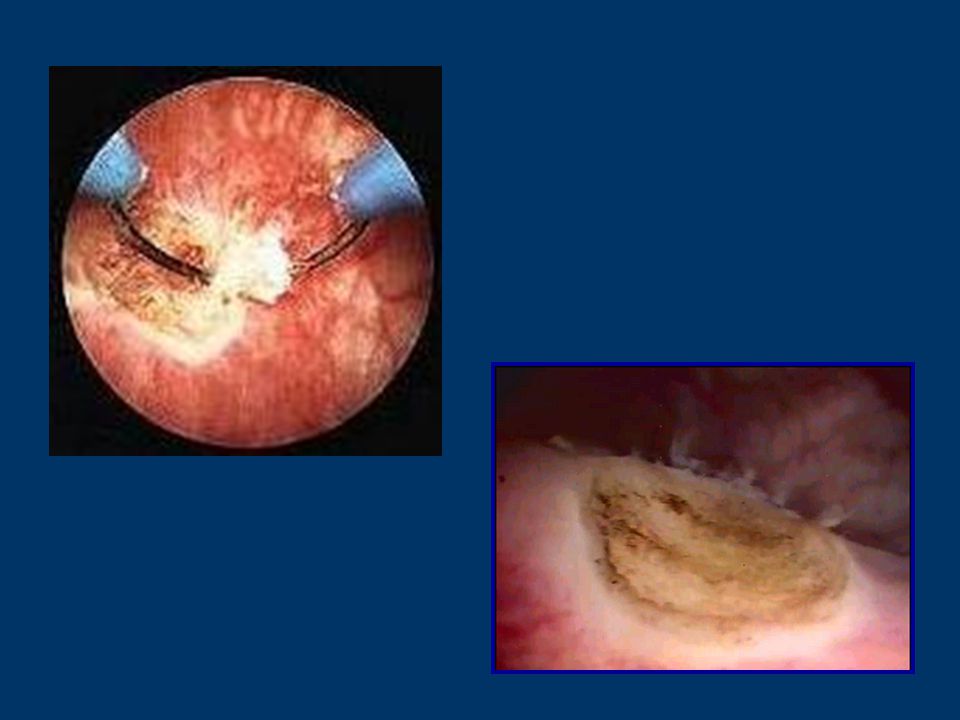
CISTOSCOPIA Cistoscopia diagnostica + Biopsia
Lesioni esofitiche Tis

21
STADIAZIONE TURBT (TransUrethral Resection of Bladder Tumor)
")
23
TERAPIA Tumori Superficiali (Ta, T1)
TURBT pTa (G1, G2) Vigile attesa Chemioterapia endocavitaria (Epirubicina, Farmorubicina, Mitomicina C) pT1 (G1, G2) Immunoterapia endocavitaria (BCG, IL-2) pT1-G3, Tis 2° TUR (Re-staging) dopo 1 mese
 Vigile attesa. Chemioterapia endocavitaria (Epirubicina, Farmorubicina, Mitomicina C) pT1 (G1, G2) Immunoterapia endocavitaria (BCG, IL-2) pT1-G3, Tis 2° TUR (Re-staging) dopo 1 mese.")
24
FOLLOW UP Tumori Superficiali
Cistoscopia: 1° anno - 1° dopo 3 mesi - ogni 3 mesi (High risk) - ogni 6 mesi (Low risk) 2°- 4° anno - ogni 4 – 9 mesi > 5° anno - ogni 6 mesi (High risk) - ogni 12 mesi (Low risk)
 - ogni 6 mesi (Low risk) 2°- 4° anno - ogni 4 – 9 mesi. > 5° anno - ogni 6 mesi (High risk) - ogni 12 mesi (Low risk)")
25
FOLLOW UP Tumori Superficiali
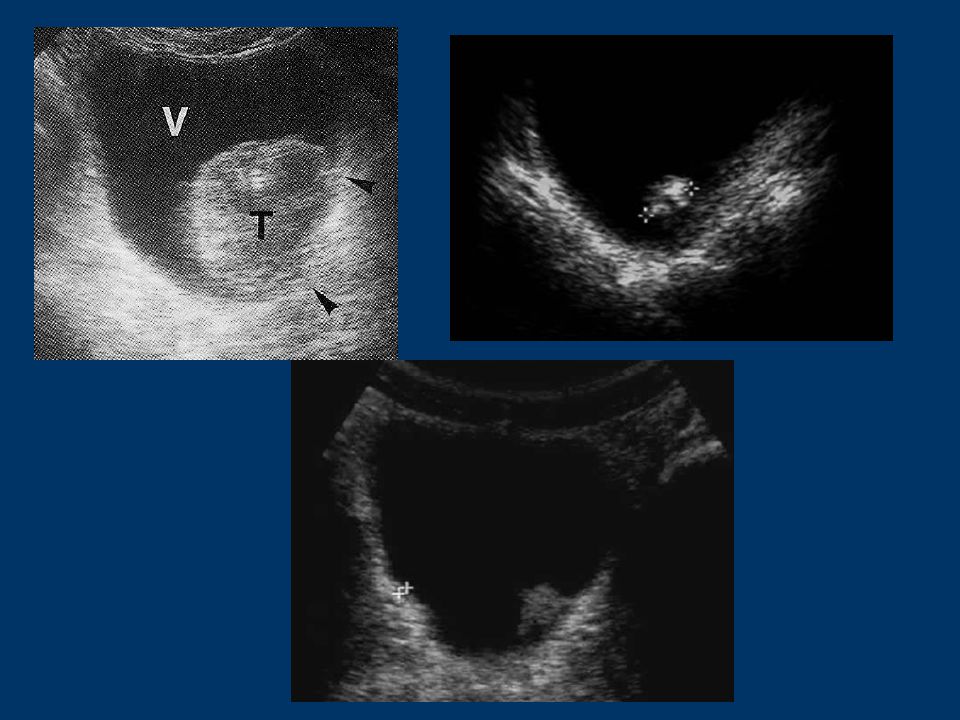
Altre indagini: Citologia Urinaria Es. delle urine completo Ecografia reni e vie urinarie Markers (UBCr, BTA, NMP-22, FISH) Cistoscopia Urografia, TC spirale
 Cistoscopia. Urografia, TC spirale.")
26
FOLLOW UP Tumori Infiltranti
Altre indagini: Citologia Urinaria Es. delle urine completo Ecografia reni e vie urinarie Markers (UBCr, BTA, NMP-22, FISH) R. Intraluminale R. Locale R. a distanza R. Locoregion. Uretroscopia, Cistoscopia TC, RMN, PET Ureteroscopia Rettoscopia, clisma Scintigrafia Urografia, TC TC, RMN, PET Biopsia
 R. Intraluminale R. Locale R. a distanza R. Locoregion. Uretroscopia, Cistoscopia TC, RMN, PET. Ureteroscopia Rettoscopia, clisma Scintigrafia. Urografia, TC TC, RMN, PET Biopsia.")
27
“Linee Guida in diagnostica per immagini”
Agenzia per i Servizi Sanitari Regionali Conferenza Stato-Regioni , 28 ottobre 2004

28
RECOMMENDATIONS 1. Mandatory evaluations
• Physical examination (including digital rectal and pelvic examination) • Renal and bladder ultrasonography and/or IVP • Cystoscopy with description of the tumour: size, site, appearance (a diagram of the bladder should be included) • Urinalysis • Urinary cytology • TUR with: – biopsy of the underlying tissue – random biopsies in the presence of positive cytology, large or non-papillary tumour – biopsy of the prostatic urethra in cases of Tis or suspicion of it 2. When the bladder tumour is muscle infiltrative and radical treatment is indicated, the following tests are mandatory • Chest X-ray • IVP and/or abdominal/pelvic CT scan • Liver ultrasonography • Bone scan if symptoms are present or alkaline phosphatase level is elevated Eau Guidelines, 2006
 • Renal and bladder ultrasonography and/or IVP. • Cystoscopy with description of the tumour: size, site, appearance. (a diagram of the bladder should be included) • Urinalysis. • Urinary cytology. • TUR with: – biopsy of the underlying tissue. – random biopsies in the presence of positive cytology, large or. non-papillary tumour. – biopsy of the prostatic urethra in cases of Tis or suspicion of it. 2. When the bladder tumour is muscle infiltrative and radical treatment is indicated, the following tests are mandatory. • Chest X-ray. • IVP and/or abdominal/pelvic CT scan. • Liver ultrasonography. • Bone scan if symptoms are present or alkaline phosphatase level is elevated. Eau Guidelines,")
Presentazioni simili





>")









>")





