Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
EROSIONE INTRALUMINALE BANDING

2
Bendaggio Gastrico Regolabile Migrazione Intragastrica
TRATTAMENTO LAPAROTOMICA LAPAROSCOPICA ENDOSCOPICA LAPAROSCOPICO + ENDOSCOPICO RIMOZIONE BANDING

3
Complicanze Rimozione Endoscopica
Torsione multipla del filo guida in esofago con successivo arresto a livello del cardias. Impossibilità di rimozione endoscopica per tenaci aderenze perigastriche. Pneumoperitoneo sintomatico senza evidenza di perforazione. P. Sakai; F. Yuji Hondo; E. Luiz de Almeida Artifon; R. Kuga; S. Ishioka Symptomatic Pneumoperitoneum after Endoscopic Removal of Adjustable Gastric Band Obesity Surgery, 2005; 15: E. Lattuada, M.A. Zappa, E. Mozzi, G. Fichera, P. Granelli, F. De Ruberto, I. Antonini,S. Radaelli, G. Roviaro Band Erosion Following Gastric Banding: How to Treat It Obesity Surgery, 2007; 17,

4
ENDOSCOPIA E FISTOLE

5
TRATTAMENTO OPZIONI TRATTAMENTO CONSERVATIVO SUTURA ENDOSCOPICA CLIP
COLLA DI FIBRINA (SE RECIDIVA) GEL PIASTRINICO POSIZIONAMENTO DI STENT OVESCO CHIRURGIA Deitel M, Crosby RD, Gagner M. The First International Consensus Summit for Sleeve Gastrectomy (SG), New York City,October 25–27, Obes Surg. 2008;18:487–96
 GEL PIASTRINICO. POSIZIONAMENTO DI STENT. OVESCO. CHIRURGIA. Deitel M, Crosby RD, Gagner M. The First International Consensus Summit for Sleeve Gastrectomy (SG), New York City,October 25–27, Obes Surg. 2008;18:487–96.")
6
TRATTAMENTO CONSERVATIVO
DRENAGGIO, NUTRIZIONE, PPI Elevati costi, ridotta probabilità di successo PAPAVRAMIDIS (J Gastroent, 2008) ATTESA UNA SETTIMANA ALTRIMENTI ENDOSCOPIA = stent
 ATTESA UNA SETTIMANA ALTRIMENTI. ENDOSCOPIA = stent.")
7
COMPLICANZE DELLO STENT
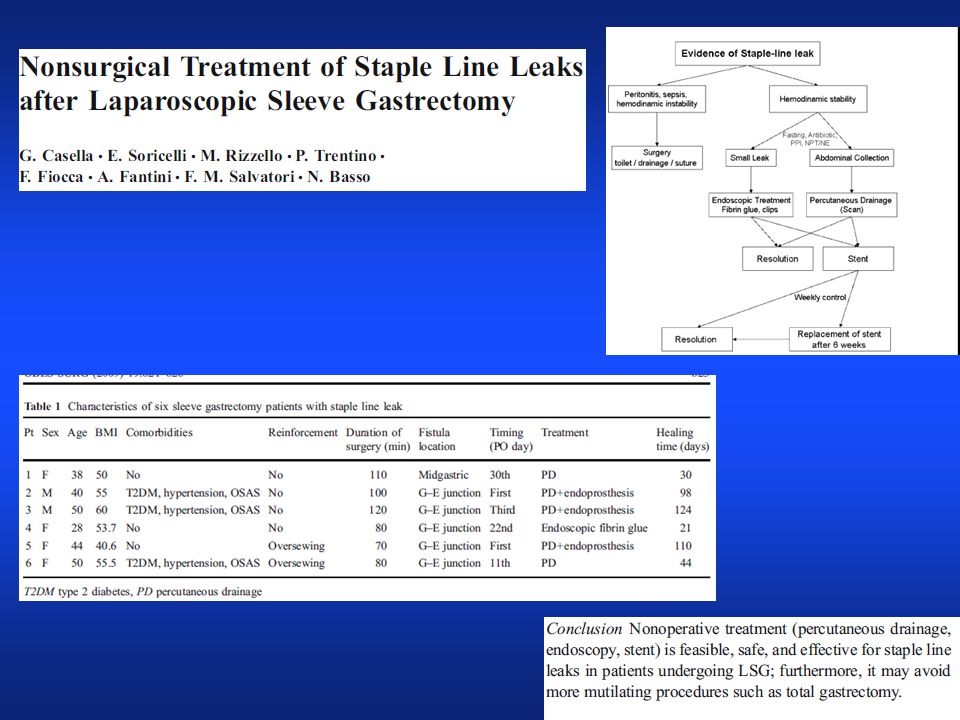
La migrazione dello stent rappresenta la complicanza più frequente, riportata nel 30% dei casi in alcuni lavori e fino al 42-58% dei casi in altri Nguyen NT, Nguyen X-MT, Dholakia C. The use of endoscopic stent in management of leaks after sleeve gastrectomy Obes Surg 2010;20: Casella G, Soricelli E, Rizzello M et al. Nonsurgical Treatment of Staple Line Leaks after Laparoscopic Sleeve Gastrectomy Obes Surg 2009;19: A volte la rimozione dello stent migrato può essere difficoltosa. In Letturatura è stato documentato un caso di stripping di mucosa esofagea durante rimozione di stent migrato con successiva gastrectomia. Serra C.,Baltasar A., Andreo L., Perez N.et al Treatment of gastric leaks with coated sel-expanding stents after sleeve gastrectomy Obes. Surg. 2007, 17( 7) : , .
 : , .")
8
COMPLICANZE DELLO STENT
A lungo termine lo stent fallisce in quanto si viene a creare del tessuto fibroso cronico intorno ad esso tale da determinare la formazione di cavità endocistica che necessita la rimozione dello stesso. Gastric Leak After Laparoscopic Sleeve Gastrectomy:Early Covered Self-Expandable Stent Reduces Healing TimeF. Simon & I Obesity Surg :687–692 Un altro limite dello stent è la ridotta tolleranza che necessita la sua successiva rimozione. Serra C, Baltasar A, Andreo L, et al. Treatment of gastric leaks with coated self-expanding stents after sleeve gastrectomy Obesity Surg. 2007;17:866–72

9
Gastrointestinal Endoscopy, February 2012
9

10
bowel migration . There was no mortality.
Immediate symptomatic improvement occurred in 90% (91% of acute leaks, 100% of fistulas, and 84% of strictures). Oral feeding was started in 79% of patients immediately after stenting. Resolution of leak or stricture after stent treatment occurred in 16 of 19 patients (84%). Healing of leak, fistula, and stricture occurred at means of 33 days, 46 days, and 7 days, respectively. Three patients (1 with leak, 1 with fistula, and 1 with stricture) had unsuccessful stent treatment. Migration of the stent occurred in 58% of 34 stents placed. Most migration was minimal, but 3 (11,3%) stents were removed surgically after distal small bowel migration . There was no mortality. 10
. Oral feeding was started in 79% of patients immediately after stenting. Resolution of leak or stricture after stent treatment occurred in 16 of 19 patients (84%). Healing of leak, fistula, and stricture occurred at means of 33 days, 46 days, and 7 days, respectively. Three patients (1 with leak, 1 with fistula, and 1 with. stricture) had unsuccessful stent treatment. Migration of the stent occurred in 58% of 34 stents. placed. Most migration was minimal, but 3 (11,3%) stents were removed surgically after distal small. bowel migration . There was no mortality. 10.")
11
TRATTAMENTO ENDOSCOPIA STENT EUBANKS, J Am Coll Surg, 2008
84% SUCCESSO - 40% MIGRAZIONE E RE STENT 2 /13 (15%) RIMOZIONE LAPAROSCOPICA DI STENT MIGRATI NELL’INTESTINO EISENDRATH, Endoscopy 2007= 75% SUCCESSO SERRA, Obes Surg, 2007 = 83% SUCCESSO
 RIMOZIONE LAPAROSCOPICA DI STENT MIGRATI NELL’INTESTINO. EISENDRATH, Endoscopy 2007= 75% SUCCESSO. SERRA, Obes Surg, 2007 = 83% SUCCESSO.")
12
TRATTAMENTO CHIRURGIA
5 fistole (27%) in sede dell’angolo di His hanno richiesto una gastrectomia totale dopo aver tentato, invano trattamenti conservativi con stent, colla etc SERRA, Obes Surg, 2006
 in sede dell’angolo di His hanno richiesto. una gastrectomia totale dopo aver tentato, invano trattamenti. conservativi con stent, colla etc. SERRA, Obes Surg,")
14
Over the Scope Clip, OTSC System®
TRATTAMENTO OVESCO Over the Scope Clip, OTSC System®

15
ENDOSCOPIA E STUDIO STOMACO ESCLUSO

16
Bypass gastrico senza esclusione dello stomaco laparotomico
Lo stomaco è escluso al transito solo funzionalmente Possibilità di studio tradizionale Immagine endoscopica

17
Importanza dello stomaco escluso
GASTRITI METAPLASIA INTESTINALE EMORRAGIE PATOLOGIE CHIRURGICHE: PERFORAZIONI E TUMORI GASTRICI “BYPASS OBSTRUCTION” NECESSITA’ DI STUDIO DELLO STOMACO ESCLUSO Spettro di manifestazioni cliniche conseguenza di una gastrectasia, solitamente perioperatoria, che può arrivare alla perforazione dello stomaco escluso

18
Bypass gastrico senza esclusione dello stomaco laparotomico
Studio endoscopico dell’anastomosi intestinale con possibilità di utilizzo delle clip per bloccare episodio emorragico

Presentazioni simili