Scaricare la presentazione
La presentazione è in caricamento. Aspetta per favore

1
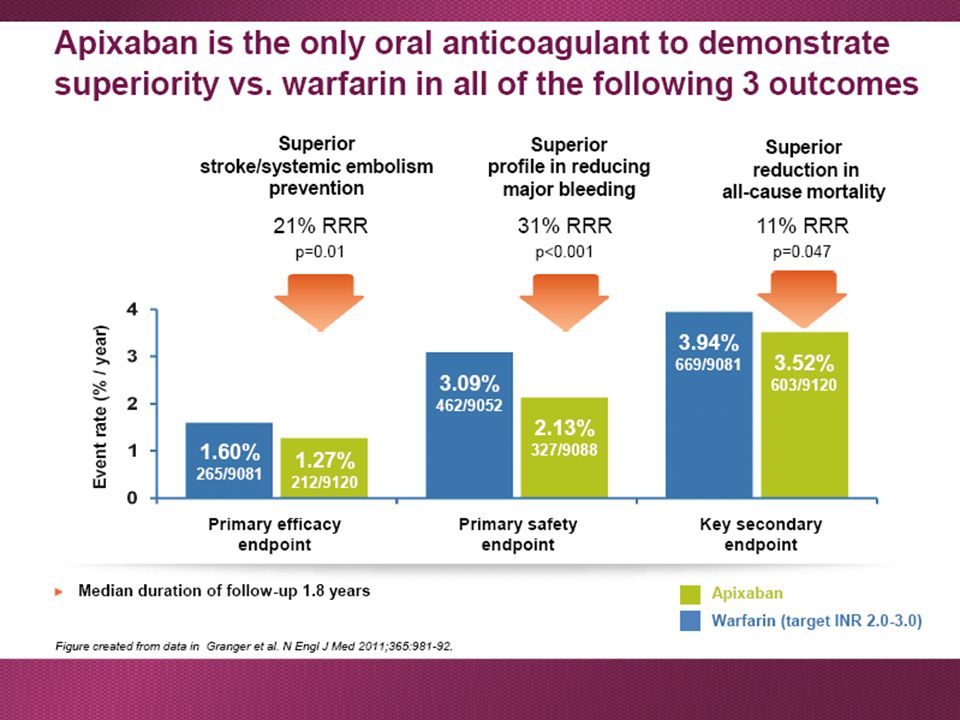
Le nuove indicazioni terapeutiche per la gestione del paziente complesso
I NAO sono tutti uguali per efficacia e sicurezza? Istruzioni per l’uso. Dott. Sergio Agosti Dirigente Medico SOC Cardiologia Ospedale Novi Ligure Hotel Il Carrettino, Tortona (Al) 15 ottobre 2015
 15 ottobre")
2
Assume that NAOs have been on the market for 5 year
A new drug comes to the market. Compared to NAOs, the new drug has: - cheaper - antidote - requirement for monthly monitoring to adjust dose - many food and drug interactions - 25% increased relative risk of stroke/systemic embolism - nearly 50% increased relative risk of major bleeding - approx. 2.5 times the rate of ICH - 10% increased relative risk of mortality Would Warfarin be approved by regulatory authorities now?

3
TAO e NAO nell’FA in Italia
Warfarin: 1960 Dabigatran (Pradaxa): giugno 2013 Rivaroxaban (Xarelto): agosto 2013 Apixaban (Eliquis): gennaio 2014 Edoxaban (Lixiana): 2016?
: giugno Rivaroxaban (Xarelto): agosto Apixaban (Eliquis): gennaio Edoxaban (Lixiana): 2016")
4
NAO in numeri…. 180000 pz nei trials
6200 articoli - studi clinici (PUBMED) Almeno pz nei registri Anticoagulante che ha più analisi post hoc, registri e articoli e pz trattati nel mondo…. Oltre 18 milioni di pz trattati nel mondo
 Almeno pz nei registri. Anticoagulante che ha più analisi post hoc, registri e articoli e pz trattati nel mondo…. Oltre 18 milioni di pz trattati nel mondo.")
5
Monosomministrazione….

6
An effective antithrombotic treatment could combine in any single patient …..
Efficacy at preventing stroke in AF and at treating DVT or PE Adherence taken as instructed for the prescribed period of time Convenience easy to take and to administer i.e. number of doses Treatment goal Safety/tolerability profile similar to control treatment 6 6

7
Assorbimento e metabolismo dei NAO
Dabigatran Rivaroxaban Apixaban Bio-disponibilità 3-7% 66% (senza cibo), 100% con il cibo 50% Pro-farmaco Si No Clearance non renale/renale 20/80% 65/35% 73/27% Metabolismo epatico(CYP3A4 involved) Si (eliminazione) Si (eliminazione, contributo minimo del CYP3A4) Assorbimento con il cibo Nessun effetto +39% Assunzione con il cibo raccomandata Mandatoria Assorbimento con H2B/PPI –12–30% Etnia Asiatica +25% Tollerabilità GI Dispepsia 5–10% Nessun problema Emivita di eliminazione 12–17 ore 5–9 ore (giovani), 11–13 ore (anziani) 12 ore Ricavata da Heidbuchel et al. Europace. 2013;15:625–651. 1. Heidbuchel et al. Europace. 2013;15:625–651.
, 100% con il cibo. 50% Pro-farmaco. Si. No. Clearance non renale/renale. 20/80% 65/35% 73/27% Metabolismo epatico(CYP3A4 involved) Si (eliminazione) Si (eliminazione, contributo minimo del CYP3A4) Assorbimento con il cibo. Nessun effetto. +39% Assunzione con il cibo raccomandata. Mandatoria. Assorbimento con H2B/PPI. –12–30% Etnia Asiatica. +25% Tollerabilità GI. Dispepsia 5–10% Nessun problema. Emivita di eliminazione. 12–17 ore. 5–9 ore (giovani), 11–13 ore (anziani) 12 ore. Ricavata da Heidbuchel et al. Europace. 2013;15:625– Heidbuchel et al. Europace. 2013;15:625–651.")
8
Adapted from European Heart Journal doi:10.1093/eurheartj/ehs253
SINTESI: efficacia e sicurezza dei nuovi anticoagulanti orali nella fibrillazione atriale non valvolare

10
Overview sui dati di sicurezza
nei trials di fase III Hazard ratio (95% CI) Study Drug Discontinuation: study drug vs. warfarin (%) Major bleeding Intracranial bleeding Gastrointestinal Side effects occurring significantly more in study drug vs. warfarin (%) ROCKET AF Rivaroxaban 20 mg od* 23.7 vs. 22.2 1.04 (0.90–1.20) p = 0.58 0.67 (0.47–0.93) p = 0.02 1.45† Epistaxis vs. 8.55, p < 0.05; haematuria 4.16 vs. 3.40, p < 0.05 RE-LY Dabigatran 150 mg bid 110 mg bid 21.2 vs. 16.6 20.7 vs. 16.6 0.93 (0.81–1.07) p = 0.31 0.80 (0.69–0.93) p = 0.003 0.40 (0.27–0.60) p < 0.001 0.31 (0.20–0.47) 1.50 (1.19–1.89) 1.10 (0.86–1.41) p = 0.43 Dyspepsia 11.3 vs. 5.8, Dyspepsia 11.8 vs. 5.8, ARISTOTLE Apixaban 5 mg bid‡ 25.3 vs. 27.5 0.69 (0.60–0.80) 0.42 (0.30–0.58) 0.89 (0.70–1.15) p = 0.37 No breakdown of adverse events provided, but total adverse events occurred in almost equal proportions Harris K and Mant J, Int J Clin Pract Jul;67(7):647-55
 Study. Drug. Discontinuation: study drug vs. warfarin (%) Major bleeding. Intracranial. bleeding. Gastrointestinal. Side effects occurring. significantly more in study drug vs. warfarin (%) ROCKET AF. Rivaroxaban. 20 mg od* 23.7 vs (0.90–1.20) p = (0.47–0.93) p = † Epistaxis vs. 8.55, p < 0.05; haematuria 4.16 vs. 3.40, p < RE-LY. Dabigatran. 150 mg bid. 110 mg bid vs vs (0.81–1.07) p = (0.69–0.93) p = (0.27–0.60) p < (0.20–0.47) 1.50 (1.19–1.89) 1.10 (0.86–1.41) p = Dyspepsia 11.3 vs. 5.8, Dyspepsia 11.8 vs. 5.8, ARISTOTLE. Apixaban. 5 mg bid‡ 25.3 vs (0.60–0.80) 0.42 (0.30–0.58) 0.89 (0.70–1.15) p = No breakdown of. adverse events. provided, but total adverse events occurred in almost. equal proportions. Harris K and Mant J, Int J Clin Pract Jul;67(7):")
11
Sanguinamenti intracranici
70% RRR relative risk reduction

12
Ictus emorragico (TF receptor)
Tissue factor (TF) is a transmembrane receptor for Factor VII/VIIa (FVII/VIIa). It is constitutively expressed by cells surrounding blood vessels. The endothelium physically separates this potent "activator" from its circulating ligand FVII/FVIIa and prevents inappropriate activation of the clotting cascade. Breakage of the endothelial barrier leads to exposure of extravascular TF and rapid activation of the clotting cascade. TF is also expressed in certain tissues, such as the heart and brain, and provides additional hemostatic protection to these tissues. Mackmann, Anesth Analg May; 108(5): The role of tissue factor and factor VIIa in hemostasis.
 is a transmembrane receptor for Factor VII/VIIa (FVII/VIIa). It is constitutively expressed by cells surrounding blood vessels. The endothelium physically separates this potent activator from its circulating ligand FVII/FVIIa and prevents inappropriate activation of the clotting cascade. Breakage of the endothelial barrier leads to exposure of extravascular TF and rapid activation of the clotting cascade. TF is also expressed in certain tissues, such as the heart and brain, and provides additional hemostatic protection to these tissues. Mackmann, Anesth Analg May; 108(5): The role of tissue factor and factor VIIa in hemostasis.")
13
Quali pazienti Il paziente anziano
Il paziente con Insufficienza Renale Il paziente con elevato rischio di sanguinamento Il paziente con valvulopatia apixaban a chi…

14
Apixaban nel paziente anziano

21
Il rischio di stroke nella FA aumenta con l’età
Warfarin è particolarmente sottoutilizzato nei pazienti anziani Halvorsen et al. Eur Hear J. 2014;35(28):1864–72; 2
:1864–72; 2.")
22
ARISTOTELE: efficacia e sicurezza in base all’età
Halvorsen et al. Eur Hear J. 2014;35(28):1864–72; 2
:1864–72; 2.")
23
Apixaban vs Warfarin nei pazienti > 80 anni
Halvorsen et al. Eur Hear J. 2014;35(28):1864–72; 2
:1864–72; 2.")
24
Apixaban nel paziente con insufficienza renale

25
IRC è comune tra i pazienti con FA
IRC aumenta il rischio di stroke, sanguinamento e morte per tutte le cause nei pazienti con FA Olesen et al. N Engl J Med 2012;367:625–35.

26
Apixaban è eliminato attraverso multiple vie di escrezione

27
Apixaban è stato più efficace e si è associato a minori
sanguinamenti maggiori vs Warfarin nei pazienti con IR Hohnloser et al. Eur Heart J 2012;22:2821–30.

28
Raccomandazioni dell’ESC nei pazienti con IR

29
Raccomandazioni dell’EHRA nei pazienti con IR (2015)
")
30
Change in GFR (CKD-EPI) Assigned to D110, D150 or Warfarin
-1 -2 -3 -4 Change from Baseline 3 6 9 12 15 18 21 30 24 27 Months *p< vs warfarin * * DE 110mg bid DE 150mg bid Warfarin * Available patients 3 months 6 months 12 months 24 months 30 months DE 110mg bid 5130 5000 4686 3368 1672 DE 150mg bid 5171 5005 4696 3434 1685 Warfarin 5243 5146 4895 3519 1703 Michael Böhm, ESC 2014, Barcelona, 30 Aug - 3 Sep 2014

31
Backgroun: Vitamin K-Antagonists Induce Vascular Damage
Price et al, Arterioscler Thromb Vasc Biol 18 (1998): Schurgers et al, Blood 109 (2007): Brodsky et al, Kidney Int 109 (2011): Krüger et al, Arterioscler Thromb Vasc Biol 33 (2013):
: Schurgers et al, Blood 109 (2007): Brodsky et al, Kidney Int 109 (2011): Krüger et al, Arterioscler Thromb Vasc Biol 33 (2013):")
32
Apixaban nel paziente con valvulopatia

33
Definizione di FA non valvolare (FAVN)
Updated EHRA Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with NVAF: Heidbuchel, August 31, 2015

34
ESC Congress 2013, Dr Alvaro Avezum, Duke Clinical Research Institute
VHD in ARISTOTLE 4808 (26,4%) patients had a history of VHD at baseline Any VHD* 4.808 100.0% Any mitral valve disease 3.578 74.4 Mitral regurgitation 3.526 73.3 Mitral stenosis 131 2.7 Any aortic valve disease 1.150 23.9 Aortic stenosis 887 18.4 Aortic regurgitation 384 8.0 Tricuspidal regurgitation 2.124 44.2 Prior valve surgery 251 5.2 ESC Congress 2013, Dr Alvaro Avezum, Duke Clinical Research Institute
 patients had a history of VHD at baseline. Any VHD* % Any mitral valve disease Mitral regurgitation Mitral stenosis Any aortic valve disease Aortic stenosis Aortic regurgitation Tricuspidal regurgitation Prior valve surgery ESC Congress 2013, Dr Alvaro Avezum, Duke Clinical Research Institute.")
35
ESPERIENZA DELL’OSPEDALE DI NOVI LIGURE NAO
TOTALE 722 pz

36
ESPERIENZA DELL’OSPEDALE DI NOVI LIGURE APIXABAN
166 pazienti in Apixaban 56% uomini - 44% donne Età media 78.2 anni (range 55-96) Primo paziente trattato il 11 settembre 2013 87% Piemonte - 13% Liguria CHADSVASC medio 4.1 (range 1-8) HASBLED medio 2.3 (range 0-5) Età media rely è 71 anni!!
 Primo paziente trattato il 11 settembre % Piemonte - 13% Liguria. CHADSVASC medio 4.1 (range 1-8) HASBLED medio 2.3 (range 0-5) Età media rely è 71 anni!!")
37
ESPERIENZA DELL’OSPEDALE DI NOVI LIGURE
Scompenso cardiaco 28% Ipertensione arteriosa 89% Diabete 22% Pregresso ictus 12% Pregressa CAD 28% Pregresso sanguinamento significativo 10% Terapia concomitante con ASA 4% Switch da TAO 28% di questi 60% con INR labile 1-2 FACEVA WARFARIN E DI QUESTI TTR 66% (nel rely e aristotele TTR 64%, nel rocket era 55%). Pregressa TAO nel rely era 50% Nel rely chads era 2.1 medio
. Pregressa TAO nel rely era 50% Nel rely chads era 2.1 medio.")
38
CHADSVASC MEDIO 4.1 CHADSVASC
NESSUNO HA CHADS 0 OVVIAMENTE E SOLO 1.8%HA CHADS DI 1, IL 12% HA CHADS 2 E IL RIMANNETE 86% HA CHADS > O UGUALE A 3… PAZIENTE AD ALTO RISCHIO DI ICTUS CHADSVASC

39
Come abbiamo somministrato Apixaban?
5 MG BID 43% (70 PZ) Età media 83 anni (range 66-96) Cl creat media 46 ml/min (range ) Se vedete l’età media dei pazienti che prendono 5 è molto più alta dei pazienti che prendono il 10, ma ci sono pazienti di 92 anni che prendono 10 mg (nello specifico abbiamo dato il 10 mg a 38 pazienti over 80 cioè al 40% circa di quelli che prendono il 10 mg, questo deriva dai differenti criteri di somministrazione dei dosaggi dell’eliquis verso dabi). Il paziente che prende 2.5 con 110 di clearance lo fa perché ha avuto grave ematuria in pradaxa ed è uno switch. 10 MG BID 57% (96 PZ) Età media 74 anni (range 52-92) Cl creat media 81 ml/min (range )
 Età media 83 anni (range 66-96) Cl creat media 46 ml/min (range ) Se vedete l’età media dei pazienti che prendono 5 è molto più alta dei pazienti che prendono il 10, ma ci sono pazienti di 92 anni che prendono. 10 mg (nello specifico abbiamo dato il 10 mg a 38 pazienti over 80 cioè al 40% circa di quelli che prendono il 10 mg, questo deriva dai differenti criteri di somministrazione dei dosaggi dell’eliquis verso dabi). Il paziente che prende 2.5 con 110 di clearance lo fa perché ha avuto grave ematuria in pradaxa ed è uno switch. 10 MG BID 57% (96 PZ) Età media 74 anni (range 52-92) Cl creat media 81 ml/min (range )")
40
STADIO CHADSVASC CON LE DUE DOSI DI APIXABAN
% PAZIENTI DATo Già PRESENTE NEL REGISTRO DANESE PER PRADAXA: NEI PAZIENTI CON CHADSVASC 2 (A Più BASSO RISCHIO TROMBOTICO) TENDIAMO A DARE DI Più IL 10, MENTRE NEI PAZIENTI A PiU’ ALTO RISCHIO TROMBOTICO TENDIAMO A DARE DI Più IL 5. QUESTO perché SONO A PAZIENTI A MAGGIOR RISCHIO (più alta età, comorbidità o che prendono farmaci concomitanti), maggiore fragilità. AL CRESCERE DELLA FRAGILITà DEL PAZIENTE TESTIMONIATA DALL’ELEVATO CHADSVASC CRESCE PROPORZIONALMENTE IL DOSAGGIO DEL 5, VEDETE COME NELLA FASCIA CON CHADS>3 LA STRAGRANDE MAGGIORANZA DEI PAZIENTI PRENDE IL 5 (78%) CHADSVASC
 TENDIAMO A DARE DI Più IL 10, MENTRE NEI PAZIENTI A PiU’ ALTO RISCHIO TROMBOTICO TENDIAMO A DARE DI Più IL 5. QUESTO perché SONO A PAZIENTI A MAGGIOR RISCHIO (più alta età, comorbidità o che prendono farmaci concomitanti), maggiore fragilità. AL CRESCERE DELLA FRAGILITà DEL PAZIENTE TESTIMONIATA DALL’ELEVATO CHADSVASC CRESCE PROPORZIONALMENTE IL DOSAGGIO DEL 5, VEDETE COME NELLA FASCIA CON CHADS>3 LA STRAGRANDE MAGGIORANZA DEI PAZIENTI PRENDE IL 5 (78%) CHADSVASC.")
41
CONTINUAZIONE O SOSPENSIONE DAL TRATTAMENTO
Follow up provvisorio, cominceremo a fare follow up sistematico con il rinnovo annuale… UN SOLO PAZIENTE PER EMORRAGIA SUBDURALE POST TRAUMATICA

42
FOLLOW UP medio 11 mesi Sospensione 0.6% Dispepsia 0%
Switch da Pradaxa in 6 pazienti Nessuna ischemia cerebrale Emorragie cerebrali (0,6%) Emorragie minori (1.2%) Nessuna allergia/intolleranza CVE (2.5%, 4 pz) senza complicanze Abbiamo avuto una emorragia subdurale post traumatica, e due emorragie minori (una ematuria con riduzione del dosaggio a 2.5x2 ed un ematoma alla gamba post traumatico) Ad un paziente è stato impiantato PM senza problemi, un altro ha fatto int chir per briglia aderenziale
 Emorragie minori (1.2%) Nessuna allergia/intolleranza. CVE (2.5%, 4 pz) senza complicanze. Abbiamo avuto una emorragia subdurale post traumatica, e due emorragie minori (una ematuria con riduzione del dosaggio a 2.5x2 ed un ematoma alla gamba post traumatico) Ad un paziente è stato impiantato PM senza problemi, un altro ha fatto int chir per briglia aderenziale.")
43
Conclusioni Apixaban è un farmaco efficace e sicuro e che garantisce un’ottima compliance e maneggevolezza Apixaban mantiene un beneficio clinico netto favorevole anche in diverse sottopopolazioni di pazienti fragili (anziani, IRC) Apixaban può essere utilizzato anche nei pazienti con valvolupatia
 Apixaban può essere utilizzato anche nei pazienti con valvolupatia.")
44
GRAZIE PER L’ATTENZIONE
GRAZIE PER L’ATTENZIONE Mail:

Presentazioni simili








e mostra un ritmo irregolare che varia continuamente nella forma. La frequenza ventricolare media.>")














